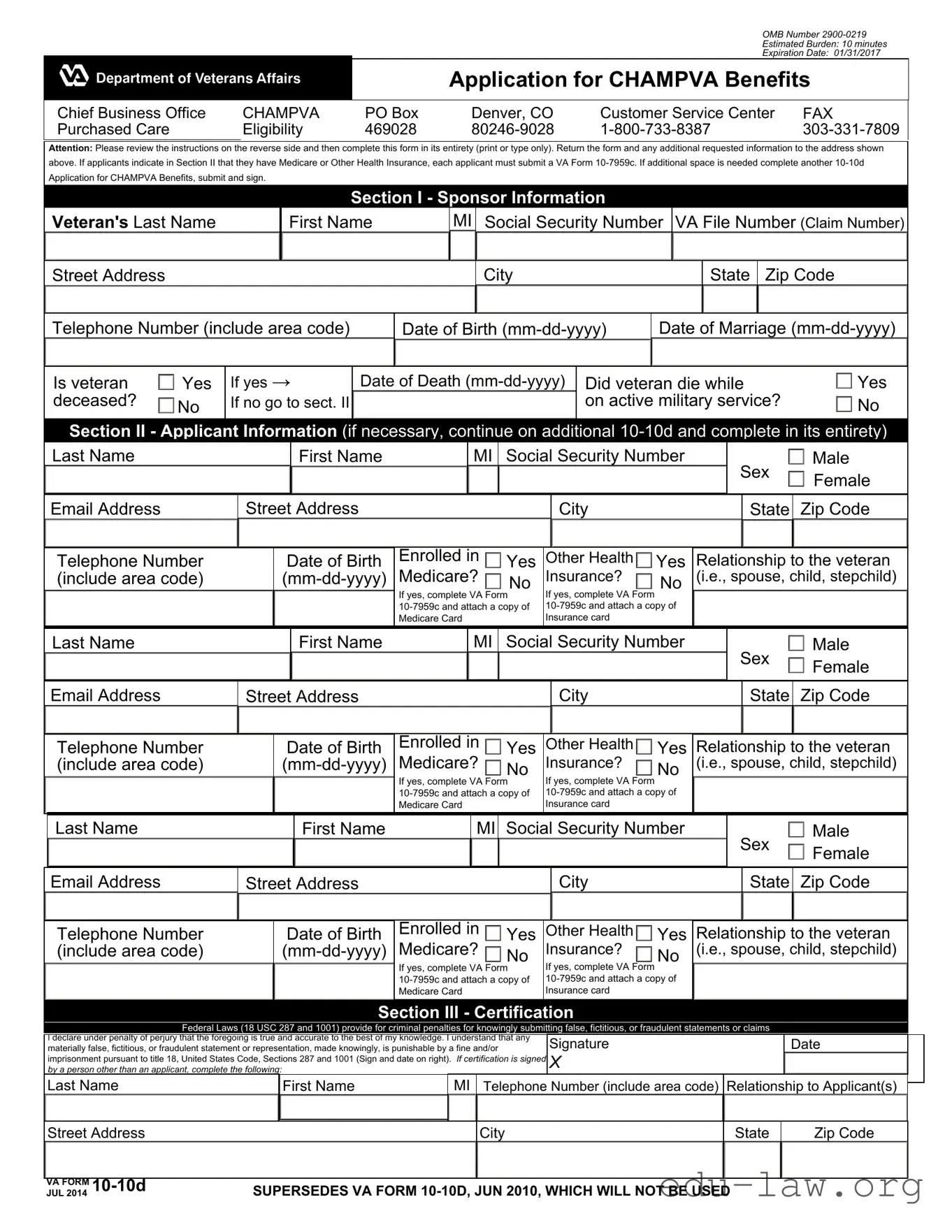
The VA Form 10-10D is a crucial document for individuals seeking CHAMPVA benefits, which provide healthcare coverage to eligible dependents of veterans. This form is designed for spouses and children of veterans who have been rated as permanently and totally disabled due to service-connected conditions, or who have died as a result of such conditions. Completing the 10-10D form requires attention to detail, as it gathers essential information about both the veteran and the applicant. The form includes sections for personal information, including names, Social Security numbers, and contact details, along with questions regarding other health insurance coverage. It is important to note that if applicants have Medicare or other health insurance, they must submit an additional form (VA Form 10-7959c) to ensure proper processing. The certification section at the end of the form emphasizes the importance of accuracy and honesty, as submitting false information can lead to serious legal consequences. Understanding the eligibility criteria and the information required can streamline the application process, making it easier for families to access the healthcare benefits they deserve.
OMB Number
Estimated Burden: 10 minutes
Expiration Date: 01/31/2017
Application for CHAMPVA Benefits
Chief Business Office |
CHAMPVA |
PO Box |
Denver, CO |
Customer Service Center |
FAX |
Purchased Care |
Eligibility |
469028 |
Attention: Please review the instructions on the reverse side and then complete this form in its entirety (print or type only). Return the form and any additional requested information to the address shown above. If applicants indicate in Section II that they have Medicare or Other Health Insurance, each applicant must submit a VA Form
Section I - Sponsor Information
|
Veteran's Last Name |
|
|
|
First Name |
|
MI |
Social Security Number |
VA File Number (Claim Number) |
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
Zip Code |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Telephone Number (include area code) |
|
Date of Birth |
|
Date of Marriage |
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Is veteran |
|
Yes |
If yes → |
|
Date of Death |
Did veteran die while |
|
|
Yes |
|
|||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
deceased? |
|
No |
If no go to sect. II |
|
|
|
|
|
|
|
|
|
|
|
|
on active military service? |
|
|
No |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Section II - Applicant |
|
Information (if |
necessary, continue on additional |
|
|||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||
|
Last Name |
|
|
|
|
|
|
First Name |
|
|
|
MI |
|
Social Security Number |
|
|
|
Sex |
|
|
Male |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
Zip Code |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Telephone Number |
|
|
|
Date of Birth |
Enrolled in |
|
|
Yes |
|
Other Health |
|
|
Yes |
Relationship to the veteran |
|
||||||||||||||||||||||
|
|
|
|
Medicare? |
|
|
Insurance? |
|
|
(i.e., spouse, child, stepchild) |
|
|||||||||||||||||||||||||||
|
(include area code) |
|
|
|
|
No |
|
No |
|
|||||||||||||||||||||||||||||
|
|
|
|
If yes, complete VA |
Form |
If yes, complete VA |
Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Medicare Card |
|
Insurance card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Last Name |
|
|
|
|
|
|
First Name |
|
|
|
MI |
|
Social |
|
Security Number |
|
|
|
Sex |
|
|
Male |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
Zip Code |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Telephone Number |
|
|
|
Date of Birth |
Enrolled in |
|
|
Yes |
|
Other Health |
|
|
Yes |
Relationship to the veteran |
|
||||||||||||||||||||||
|
|
|
|
Medicare? |
|
|
Insurance? |
|
|
(i.e., spouse, child, stepchild) |
|
|||||||||||||||||||||||||||
|
(include area code) |
|
|
|
|
No |
|
No |
|
|||||||||||||||||||||||||||||
|
|
|
|
If yes, complete VA |
|
If yes, complete VA |
Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
Form |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Medicare Card |
|
Insurance card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Last Name |
|
|
|
|
|
|
First Name |
|
|
|
|
MI |
|
Social Security Number |
|
|
|
Sex |
|
|
Male |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
Zip Code |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Telephone Number |
|
|
|
Date of Birth |
Enrolled in |
|
|
Yes |
|
Other Health |
|
|
Yes |
Relationship to the veteran |
|
||||||||||||||||||||||
|
|
|
|
Medicare? |
|
|
Insurance? |
|
|
(i.e., spouse, child, stepchild) |
|
|||||||||||||||||||||||||||
|
(include area code) |
|
|
|
|
No |
|
No |
|
|||||||||||||||||||||||||||||
|
|
|
|
If yes, complete VA |
Form |
If yes, complete VA |
Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Medicare Card |
|
Insurance card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
Section III - Certification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
Federal Laws (18 USC 287 and 1001) provide for criminal penalties for knowingly submitting false, fictitious, or fraudulent statements or claims |
|
|
|
|
|||||||||||||||||||||||||||||||
|
I declare under penalty of perjury that the foregoing is true and accurate to the best of my knowledge. I understand that any |
|
Signature |
|
|
|
|
|
|
|
|
|
|
Date |
|
|||||||||||||||||||||||
|
materially false, fictitious, or fraudulent statement or representation, made knowingly, is punishable by a fine and/or |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
imprisonment pursuant to title 18, United States Code, Sections 287 and 1001 (Sign and date on right). If certification is signed |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
by a person other than an applicant, complete the following: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Last Name |
|
|
|
|
First Name |
|
|
MI |
Telephone Number (include area code) |
Relationship to Applicant(s) |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
VA FORM |
|
|
SUPERSEDES VA FORM |
|
|
|
|
|||||||||||||||||||||||||||||||
JUL 2014 |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
Page 2 of 3
Notice: Termination of marriage by divorce or annulment to the qualifying sponsor ends CHAMPVA eligibility as of midnight on the effective date of the dissolution of marriage. Changes in status should be reported immediately to CHAMPVA, ATTN: Eligibility Unit, PO Box 469028, Denver, CO
Privacy Act Information: The authority for collection of the requested information on this form is 38 USC 501 and 1781. The purpose of collecting this information is to determine your eligibility for CHAMPVA benefits. The information you provide may be verified by a computer matching program at any time. You are requested to provide your social security number as your VA record is filed and retrieved by this number. You do not have to provide the requested information on this form but if any or all of the requested information is not provided, it may delay or result in denial of your request for CHAMPVA benefits. Failure to furnish the requested information will have no adverse impact on any other VA benefit to which you may be entitled. The responses you submit are considered confidential and may be disclosed outside VA only if the disclosure is authorized under the Privacy Act, including the routine uses identified in the VA system of records number 54VA16, titled "Health Administration Center Civilian Health and Medical Program Records
The Paperwork Reduction Act: This information collection is in accordance with the clearance requirements of section 3507 of the Paperwork Reduction Act of 1995. Public reporting burden for this collection of information is estimated to average 10 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Comments regarding this burden estimate or any other aspect of this collection, including suggestions for reducing the burden, may be addressed by calling the CHAMPVA Help Line,
Application for CHAMPVA Benefits – Important Notes and Definitions
CHAMPVA Eligibility Criteria
The following persons are eligible for CHAMPVA benefits, providing they are NOT eligible for
DoD's TRICARE benefits:
•the spouse or child of a veteran who has been rated by a VA regional office as having a permanent and total
•the surviving spouse or child of a veteran who died as a result of a
•the surviving spouse or child of a person who died in the line of duty and not due to misconduct.
Medicare Impact. If you are eligible or become eligible for Medicare Part A and you are under age 65, you MUST have Part B to be covered by CHAMPVA. Effective October 1, 2001, CHAMPVA benefits were extended to beneficiaries age 65 or older. If you are eligible for Medicare Part A and you are age 65 or older, you are required to have Part B to be covered by CHAMPVA if your 65th birthday was on or after June 5, 2001, or if you were already enrolled in Part B prior to June 5, 2001.
VA FORM JUL 2014
SUPERSEDES VA FORM
Application for CHAMPVA Benefits – Important Notes and Definitions |
Page 3 of 3 |
Eligibility Definitions
Sponsor – Refers to the veteran upon whom CHAMPVA eligibility for the applicant is based.
Spouse – Refers to a person who is married to or is a widow(er) of an eligible CHAMPVA sponsor. If you are certifying that a person is your spouse for the purpose of VA benefits, your marriage must be recognized by the place where you and/or your spouse resided at the time of marriage, or where you and/or your spouse reside when you file your claim (or at a later date when you become eligible for benefits) (38 U.S.C. 103(c)). Additional guidance on when VA recognizes marriages is available at http://www.va.gov/opa/marriage/. If the spouse remarries prior to age 55, CHAMPVA benefits end on the date of the remarriage. Effective February 4, 2003, if the spouse remarries on or after age 55, CHAMPVA benefits continue. Additionally, in some instances, a remarried surviving spouse whose remarriage is either terminated by death, divorce or annulment is CHAMPVA eligible when supported by a copy of the appropriate documentation (death certificate/divorce decree/annulment certification).
Child – Includes legitimate, adopted, illegitimate, and stepchildren. To be eligible, the child must be unmarried and: 1) under the age of 18; or 2) who, before reaching age 18, became permanently incapable of
NOTE: Except for stepchildren, the eligibility of children is not affected by divorce or remarriage of the spouse or surviving spouse.
School Certification
In order to extend CHAMPVA benefits to students age 18 to 23, school certification of
School certification letters should be on school letterhead and include:
•Student's full name
•Student's Social Security number (SSN)
•Exact beginning date and projected graduation date
•Number of semester hours or equivalent (high schools excluded)
•Certification of
School generated forms are acceptable as long as they provide the above information. While certifications submitted in a foreign language are acceptable, additional time will be required for translation. Certifications may be submitted by mail to the address on the front or by FAX
to
NOTE: It is important to notify the Chief Business Office Purchased Care of any change in student status such as withdrawal or change from
break in CHAMPVA eligibility.
VA FORM JUL 2014 |
SUPERSEDES VA FORM |
| Fact Name | Description |
|---|---|
| OMB Number | The OMB Number for the VA 10-10D form is 2900-0219. |
| Estimated Burden | Completing the form is estimated to take about 10 minutes. |
| Expiration Date | The expiration date for this form was January 31, 2017. |
| Governing Laws | The form is governed by 38 USC 501 and 1781. |
| Eligibility Criteria | Eligibility for CHAMPVA benefits includes spouses or children of veterans with service-connected disabilities. |
Completing the VA Form 10-10D is an essential step in applying for CHAMPVA benefits. After filling out the form, it must be submitted to the appropriate address along with any additional requested information. Ensure that all sections are completed accurately to avoid any delays in processing your application.
After completing all sections, review the form for accuracy. It is crucial to ensure that all required information is provided to prevent delays in processing. Once verified, submit the form and any additional documents to the address listed at the top of the form.
What is the purpose of the VA Form 10-10D?
The VA Form 10-10D is used to apply for CHAMPVA benefits, which provide health care coverage for eligible dependents of veterans. This includes spouses and children of veterans who have been rated as having a permanent and total service-connected condition or who have died as a result of such a condition. The form collects necessary information to determine eligibility for these benefits.
Who is eligible to apply for CHAMPVA benefits using this form?
Eligibility for CHAMPVA benefits extends to the spouse or child of a veteran who has been rated by a VA regional office as having a permanent and total service-connected condition. Additionally, the surviving spouse or child of a veteran who died due to a service-connected condition may also apply. It is important to note that applicants must not be eligible for DoD's TRICARE benefits to qualify.
What should I do if I have Medicare or other health insurance?
If you have Medicare or other health insurance, you must complete VA Form 10-7959c and attach it to your 10-10D application. This requirement ensures that the VA can accurately assess your health coverage and determine your eligibility for CHAMPVA benefits. Each applicant listed on the form must provide this additional information if applicable.
What happens if my marital status changes?
Any change in marital status, such as divorce or annulment, will affect your eligibility for CHAMPVA benefits. Specifically, if you divorce the qualifying sponsor, your eligibility ends at midnight on the effective date of the dissolution. It is crucial to report any changes in status immediately to the CHAMPVA Eligibility Unit to ensure that your benefits are managed appropriately.
Incomplete Information: Many applicants fail to fill out all required fields. Missing information can lead to delays or denials. Ensure every section is completed, especially personal details and relationship to the veteran.
Incorrect Submission: Some individuals submit the form without the necessary attachments, such as the VA Form 10-7959c for Medicare or other health insurance. Always check if additional forms are required based on your situation.
Signature Issues: A common mistake is not signing the form or having someone else sign without providing their relationship to the applicant. Signatures are crucial for validating the application.
Ignoring Updates: Applicants often overlook the need to report changes in marital status or eligibility. This can affect CHAMPVA benefits. Notify the CHAMPVA office immediately if there are any changes.
When applying for CHAMPVA benefits using the VA Form 10-10D, several other forms and documents may be required to complete your application process. Below is a list of commonly used forms that you might encounter.
Each of these forms plays a critical role in ensuring that your application for CHAMPVA benefits is complete and accurate. Having the right documents ready can help expedite the process and avoid potential delays.
The VA Form 10-10D is similar to the Medicare Application Form (CMS-10106) in that both are used to determine eligibility for health benefits. The Medicare application collects personal information, including Social Security numbers and date of birth, to assess whether an individual qualifies for Medicare coverage. Like the 10-10D, the Medicare form also requires applicants to provide details about their health insurance status and any other relevant medical history. Both forms aim to ensure that applicants receive the appropriate health care benefits based on their eligibility criteria.
Another document similar to the VA Form 10-10D is the TRICARE Enrollment Application. This form is used by military families to enroll in TRICARE, the health care program for military members and their dependents. Like the 10-10D, the TRICARE application requests information about the applicant’s relationship to the service member and requires details about any other health insurance coverage. Both forms serve the purpose of determining eligibility for health care benefits based on military service and family status.
The Health Insurance Marketplace Application is also comparable to the VA Form 10-10D. This application is used by individuals seeking to enroll in health insurance plans offered through the Affordable Care Act. Similar to the 10-10D, it collects personal information, including household income and family size, to determine eligibility for various health insurance options. Both applications emphasize the importance of providing accurate information to ensure that applicants receive the benefits they are entitled to.
Additionally, the Supplemental Nutrition Assistance Program (SNAP) Application shares similarities with the VA Form 10-10D. While SNAP focuses on food assistance, it also requires detailed personal information to assess eligibility. Both forms require applicants to disclose income, household composition, and other relevant factors that determine eligibility for benefits. The goal of both applications is to ensure that individuals receive support based on their specific needs.
The Medicaid Application is another document akin to the VA Form 10-10D. Medicaid provides health coverage for low-income individuals and families. The application process for Medicaid involves submitting personal and financial information, much like the 10-10D. Both forms aim to establish eligibility for health benefits, ensuring that applicants receive the necessary care based on their financial situation and health needs.
The Social Security Disability Insurance (SSDI) Application is also similar to the VA Form 10-10D. SSDI provides benefits to individuals who are unable to work due to a disability. The application requires detailed information about the applicant’s work history, medical conditions, and personal details. Both forms emphasize the importance of accurate information to determine eligibility for benefits, reflecting the need for comprehensive documentation in the application process.
Lastly, the Veterans Benefits Administration (VBA) Application for Compensation or Pension is comparable to the VA Form 10-10D. This application is used by veterans seeking financial assistance for disabilities or other service-related issues. Similar to the 10-10D, it requires personal information, including service history and medical conditions, to assess eligibility for benefits. Both forms are critical in helping veterans access the support they need based on their service and health status.
When filling out the VA Form 10-10D for CHAMPVA benefits, it is essential to approach the process with care and attention to detail. Here are six important do's and don'ts to keep in mind:
By following these guidelines, applicants can help ensure a smoother application process for CHAMPVA benefits.
This form is not exclusively for veterans. It is designed for the spouses and children of veterans who meet specific eligibility criteria. These individuals can apply for CHAMPVA benefits using this form.
While the form is a necessary step in the application process, it does not guarantee benefits. Eligibility is determined based on various factors, including the veteran's service-connected disability status and the applicant's relationship to the veteran.
Changes in marital status must be reported immediately to CHAMPVA. If a marriage is terminated by divorce or annulment, CHAMPVA eligibility ends as of the effective date of the dissolution.
Supporting documents are often required. For example, if the applicant has Medicare or other health insurance, they must submit VA Form 10-7959c along with the 10-10D form. Failing to include necessary documentation may delay the application process.
Each eligible family member must complete a separate VA Form 10-10D. If additional space is needed, applicants should fill out another form to ensure all information is accurately captured.
Filling out the VA Form 10-10D for CHAMPVA benefits is a crucial step for eligible applicants. Here are key takeaways to keep in mind:
By following these guidelines, applicants can navigate the process of applying for CHAMPVA benefits more effectively.