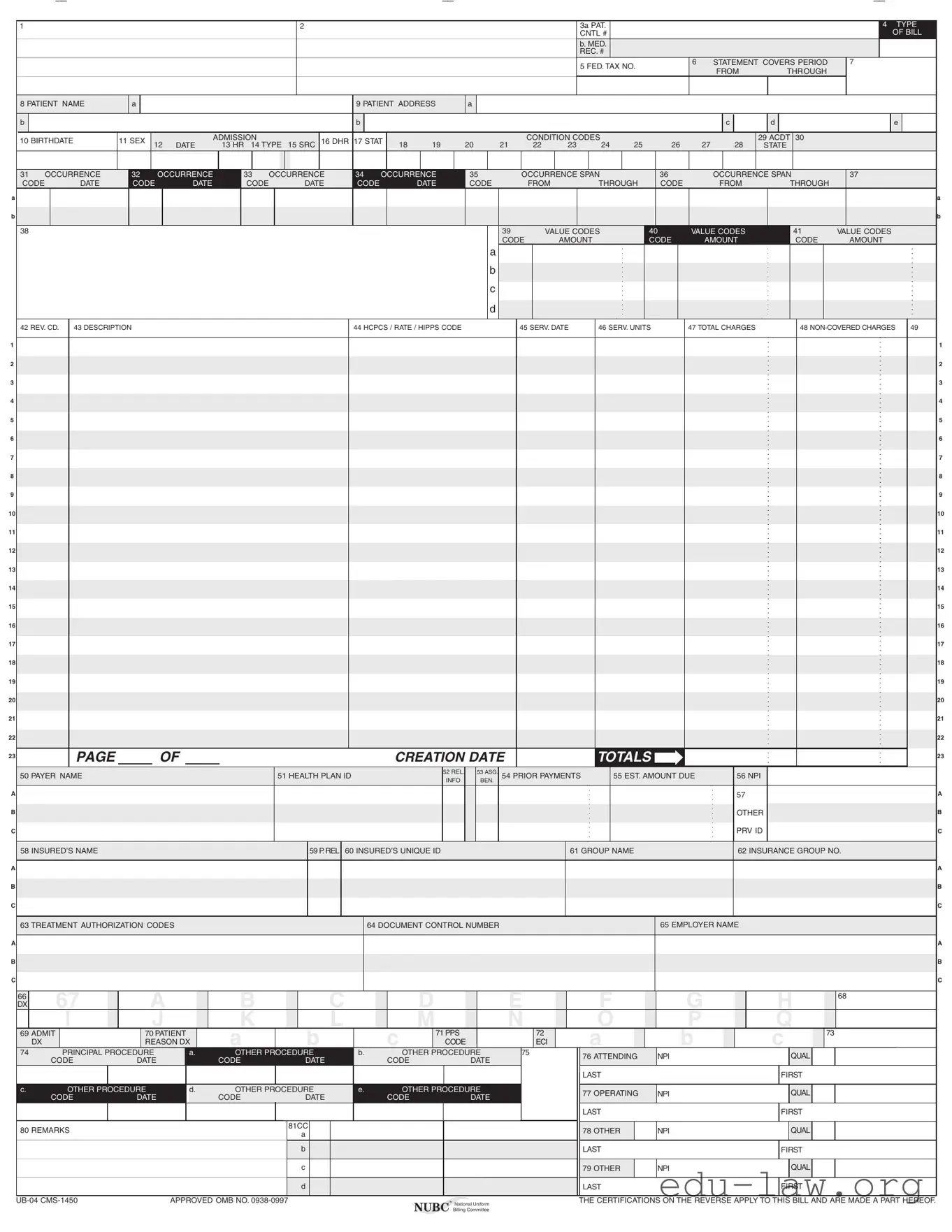
The UB-04 form, also known as the CMS-1450, is a critical document used in the healthcare industry for billing purposes. It serves as a standardized claim form for institutional providers, such as hospitals and skilled nursing facilities, to submit claims for reimbursement to Medicare, Medicaid, and other insurance payers. This form captures a wide array of information, including patient demographics, service details, and charges incurred during treatment. Key sections of the form require the inclusion of the patient’s name, address, and medical record number, as well as details about the services rendered, such as the dates of service and relevant procedure codes. Additionally, the UB-04 includes fields for reporting various condition codes, occurrence codes, and value codes that help clarify the nature of the services provided and any special circumstances surrounding the patient’s care. Understanding the structure and requirements of the UB-04 form is essential for healthcare providers to ensure accurate and timely reimbursement while complying with federal and state regulations. Proper completion of this form not only facilitates the billing process but also plays a significant role in maintaining the integrity of healthcare records and ensuring that patients receive the benefits they are entitled to.
A
B
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
A
B
C
A
B
C
A
B
C
1 |
2 |
3a PAT. |
|
|
|
|
|
4 TYPE |
|
|
CNTL # |
|
|
|
|
|
OF BILL |
|
|
b. MED. |
|
|
|
|
|
|
|
|
REC. # |
|
|
|
|
|
|
|
|
5 FED. TAX NO. |
6 |
STATEMENT COVERS PERIOD |
7 |
|
||
|
|
|
FROM |
THROUGH |
|
|
||
|
|
|
|
|
|
|
||
8 PATIENT NAME |
a |
|
|
|
|
9 PATIENT ADDRESS |
a |
|
|
|
|
|
|
|
|
|
|
||
b |
|
|
|
|
|
b |
|
|
|
|
|
|
|
|
|
|
c |
d |
e |
10 BIRTHDATE |
11 SEX |
|
|
ADMISSION |
|
16 DHR 17 STAT |
|
|
|
|
CONDITION CODES |
|
|
|
|
|
29 ACDT 30 |
|
|
12 |
DATE |
13 HR 14 TYPE |
15 SRC |
18 |
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
STATE |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31 OCCURRENCE |
32 |
|
OCCURRENCE |
33 |
OCCURRENCE |
34 |
OCCURRENCE |
35 |
|
|
|
OCCURRENCE SPAN |
|
36 |
|
|
|
OCCURRENCE SPAN |
|
37 |
|
|
|
||||||||||||||||||||||||||||||
CODE |
DATE |
CODE |
|
DATE |
CODE |
|
|
|
DATE |
CODE |
|
DATE |
CODE |
|
|
|
FROM |
THROUGH |
|
CODE |
|
|
FROM |
|
THROUGH |
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
|
|
VALUE CODES |
40 |
|
|
VALUE CODES |
|
41 |
|
VALUE CODES |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE |
|
AMOUNT |
|
|
|
CODE |
|
|
AMOUNT |
|
CODE |
|
AMOUNT |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
42 REV. CD. |
43 DESCRIPTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
44 HCPCS / RATE / HIPPS CODE |
|
|
|
|
45 SERV. DATE |
46 SERV. UNITS |
47 TOTAL CHARGES |
|
|
48 |
49 |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAGE |
|
|
OF |
|
|
|
|
|
|
|
|
|
|
CREATION DATE |
|
|
|
|
|
|
|
TOTALS |
|
|
|
|
|
|
|
|
|
|
|
|
|
23 |
|||||||||||||||
50 PAYER NAME |
|
|
|
|
|
|
|
|
51 HEALTH PLAN ID |
|
|
|
|
52 REL. |
|
53 ASG. |
54 PRIOR PAYMENTS |
|
55 EST. AMOUNT DUE |
|
|
56 NPI |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFO |
|
BEN. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
57 |
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRV ID |
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
58 INSURED’S NAME |
|
|
|
|
|
|
|
|
|
|
|
59 P. REL |
60 INSURED’S UNIQUE ID |
|
|
|
|
|
|
|
|
61 GROUP NAME |
|
|
|
|
|
|
|
62 INSURANCE GROUP NO. |
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
63 TREATMENT AUTHORIZATION CODES |
|
|
|
|
|
|
|
|
64 DOCUMENT CONTROL NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
65 EMPLOYER NAME |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C
66 |
67 |
A |
|
B |
|
C |
|
D |
|
E |
F |
G |
H |
68 |
DX |
|
|
|
|
|
|||||||||
|
I |
J |
|
K |
|
L |
|
M |
|
N |
O |
P |
Q |
|
69 ADMIT |
70 PATIENT |
|
A |
B |
|
C |
71 PPS |
|
72 |
A |
B |
C |
73 |
|
|
DX |
REASON DX |
|
CODE |
|
ECI |
|
|||||||
74 |
PRINCIPAL PROCEDURE |
a. |
OTHER PROCEDURE |
b. |
|
OTHER PROCEDURE |
75 |
76 ATTENDING |
NPI |
QUAL |
|
|||
|
CODE |
DATE |
|
CODE |
DATE |
|
CODE |
DATE |
|
|
||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
LAST |
|
FIRST |
|
c. |
OTHER PROCEDURE |
d. |
OTHER PROCEDURE |
e. |
|
OTHER PROCEDURE |
|
77 OPERATING |
NPI |
QUAL |
|
|||
|
CODE |
DATE |
|
CODE |
DATE |
|
CODE |
DATE |
|
|
||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
LAST |
|
FIRST |
|
80 REMARKS |
|
|
|
81CC |
|
|
|
|
|
78 OTHER |
NPI |
QUAL |
|
|
|
|
|
a |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b |
|
|
|
|
|
LAST |
|
FIRST |
|
|
|
|
|
|
c |
|
|
|
|
|
79 OTHER |
NPI |
QUAL |
|
|
|
|
|
|
d |
|
|
|
|
|
LAST |
|
FIRST |
|
APPROVED OMB NO. |
™ National Uniform |
THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. |
|
|
|
NUBC Billing Committee |
|
| Fact Name | Description |
|---|---|
| Form Purpose | The UB-04 form is used for billing institutional healthcare services, including hospitals and skilled nursing facilities. |
| Governing Body | The form is maintained by the National Uniform Billing Committee (NUBC). |
| Required Fields | Essential fields include patient name, admission date, and total charges. |
| Federal Compliance | Submission of the UB-04 certifies compliance with federal laws, including Medicare and Medicaid regulations. |
| State-Specific Forms | Some states require additional documentation or modifications to the UB-04 form based on local laws. |
| Submission Methods | The UB-04 can be submitted electronically or via paper, depending on the payer's requirements. |
| Certification Requirements | Submitters must certify that all information is accurate and complete to avoid penalties. |
| Common Uses | It is commonly used for inpatient and outpatient hospital services, as well as long-term care. |
| Data Elements | The form contains numerous data elements, including patient demographics, service dates, and billing codes. |
| Legal Implications | Misrepresentation on the UB-04 can lead to civil monetary penalties and criminal charges under federal and state laws. |
Filling out the UB-04 form is a crucial step in the medical billing process. Once you have gathered all necessary information, you can proceed with completing the form accurately. This ensures that the claim is processed efficiently and reduces the chances of delays or denials from insurance companies.
By following these steps, you can effectively complete the UB-04 form. This attention to detail will help facilitate a smoother claims process, ultimately benefiting both the provider and the patient.
What is the UB-04 form?
The UB-04 form, also known as the CMS-1450, is a standardized billing form used by healthcare providers to bill for services provided to patients. It is primarily utilized by hospitals and other facilities to submit claims for reimbursement from Medicare, Medicaid, and other insurance payers. The form captures essential details about the patient, the services rendered, and the charges incurred during their care.
What information is required on the UB-04 form?
The UB-04 form requires various pieces of information. This includes patient demographics like name, address, and date of birth. It also requires details about the services provided, such as dates of service, revenue codes, and total charges. Additionally, the form needs to include payer information, such as the insurance company’s name and any relevant identification numbers. Accurate completion of these fields is crucial for timely and correct reimbursement.
How do I fill out the UB-04 form correctly?
Filling out the UB-04 form correctly involves several steps. Start by gathering all necessary patient information and service details. Ensure that each section of the form is completed accurately, paying close attention to codes and descriptions. Double-check for any errors or missing information before submission. It's also essential to follow specific payer guidelines, as different insurance companies may have unique requirements regarding the form's completion.
What are the consequences of incorrect information on the UB-04 form?
Submitting incorrect information on the UB-04 form can lead to several issues. Claims may be denied or delayed, resulting in lost revenue for the healthcare provider. In some cases, misrepresentation or falsification of information could lead to civil monetary penalties or even criminal charges. Therefore, accuracy is vital when completing this form to avoid potential legal and financial repercussions.
Who is responsible for submitting the UB-04 form?
The responsibility for submitting the UB-04 form typically falls on the healthcare provider or their billing department. In many cases, hospitals and facilities have dedicated staff trained in medical billing who ensure that claims are filed correctly. However, providers may also delegate this task to third-party billing companies. Regardless of who submits the form, the healthcare provider remains accountable for the accuracy of the information provided.
Where can I find more information about the UB-04 form?
For more information about the UB-04 form, you can visit the National Uniform Billing Committee's website at http://www.nubc.org/. This site offers resources, including data element specifications and guidelines for completing the form. Additionally, many healthcare billing textbooks and online courses provide in-depth training on the UB-04 and medical billing practices.
Incorrect Patient Information: One of the most common mistakes is entering incorrect patient details, such as the name, address, or birthdate. Accurate information is crucial for processing claims smoothly.
Missing Control Numbers: Forgetting to include the control number can lead to delays. This number helps track the bill through the billing system.
Inaccurate Dates: Filling in the wrong dates, especially the service dates or coverage period, can cause issues. Ensure that all dates align with the patient’s treatment timeline.
Omitting Codes: Failing to include necessary codes, such as diagnosis or procedure codes, can result in claim denials. Each code must accurately reflect the services provided.
Inconsistent Insurance Information: Providing mismatched insurance details can lead to confusion. Always double-check that the insurance name and policy numbers are correct.
Not Signing the Form: A signature is often required to certify the information is true. Omitting this can halt the claim process.
Ignoring Payer Requirements: Each payer may have specific requirements for submission. Not adhering to these can result in rejections. Familiarize yourself with the guidelines for each payer.
Incorrect Unit Count: Miscalculating the number of service units can lead to billing errors. Ensure that the quantity matches the services rendered.
Failure to Review for Completeness: Submitting the form without a thorough review can lead to overlooked errors. Always double-check that all required fields are filled out completely.
The UB-04 form, also known as the CMS-1450, is an essential document used for billing healthcare services provided by hospitals and other facilities. When submitting this form, several other documents often accompany it to ensure a complete and accurate claim. Below are some common forms and documents that may be used alongside the UB-04.
Each of these documents plays a vital role in the claims process, helping to streamline communication between healthcare providers and insurers. By ensuring all necessary forms are included, you can facilitate a smoother billing experience and reduce the likelihood of claim denials.
The CMS-1500 form is commonly used by healthcare providers to bill Medicare and other insurance carriers for outpatient services. It captures essential patient information, diagnosis codes, and procedure codes, similar to the UB-04 form. However, the CMS-1500 is specifically designed for individual practitioners and outpatient settings, whereas the UB-04 is tailored for institutional providers like hospitals and nursing facilities.
The HCFA 1450 form, which is essentially another name for the UB-04, serves the same purpose in billing for institutional services. It includes similar data fields, such as patient demographics, service dates, and charges. The HCFA 1450 is recognized by Medicare and other payers, ensuring that institutions can effectively communicate their billing needs.
The ADA Claim Form is utilized by dental providers to submit claims for dental services. Like the UB-04, it includes fields for patient information, provider details, and specific service codes. While the UB-04 covers a broader range of healthcare services, the ADA Claim Form focuses solely on dental procedures, catering to the unique needs of dental billing.
The UB-92 form was the predecessor to the UB-04 and served a similar function in hospital billing. While both forms collect information about patient admissions, diagnoses, and charges, the UB-04 has been updated to include more comprehensive data elements and is now the standard form for institutional billing.
The 837 Institutional transaction is an electronic format used for submitting healthcare claims. Similar to the UB-04, it captures detailed information about patient services, diagnoses, and billing amounts. The 837 format allows for efficient electronic processing of claims, streamlining the billing process for institutional providers.
The Patient Encounter Form, often referred to as a superbill, is used by healthcare providers to document services rendered during a patient visit. While it serves a different purpose than the UB-04, it includes similar data elements, such as procedure codes and patient demographics. This form helps providers ensure accurate billing and coding before submitting claims to payers.
The CMS 1490S form is a Medicare claim form for patients who do not have a primary insurance. It shares similarities with the UB-04 in that it requires patient information and service details. However, it is specifically designed for patients seeking reimbursement directly from Medicare, rather than through institutional providers.
The CMS-855 form is an application for Medicare enrollment, which includes information about the healthcare provider’s practice. While it does not function as a billing form like the UB-04, it is crucial for establishing the provider’s credentials and ensuring they can bill Medicare for services rendered, thus linking it indirectly to the billing process.
The NPI application form is used by healthcare providers to apply for a National Provider Identifier. While it does not serve a billing function, having an NPI is essential for submitting claims using the UB-04. The NPI ensures that providers are accurately identified in the billing process, similar to how patient and service information is captured on the UB-04.
The UB-04 form also shares similarities with the Medicare Cost Report, which is used by hospitals to report costs associated with patient care. Both documents require detailed information about services provided and associated costs. While the UB-04 focuses on individual claims, the Medicare Cost Report provides a comprehensive overview of a provider's financial performance over a specific period.
When filling out the UB-04 form, attention to detail is crucial. Here are some essential guidelines to follow and avoid.
Understanding the UB-04 form is essential for healthcare providers and patients alike. However, several misconceptions can lead to confusion and errors in billing. Here are six common misunderstandings:
Being informed about these misconceptions can empower healthcare providers and patients alike. Understanding the nuances of the UB-04 form can lead to smoother billing processes and fewer headaches down the line.
Filling out the UB-04 form correctly is essential for healthcare providers to ensure proper billing and reimbursement. Here are five key takeaways to keep in mind:
By following these guidelines, healthcare providers can enhance their billing processes and reduce the likelihood of claim issues.