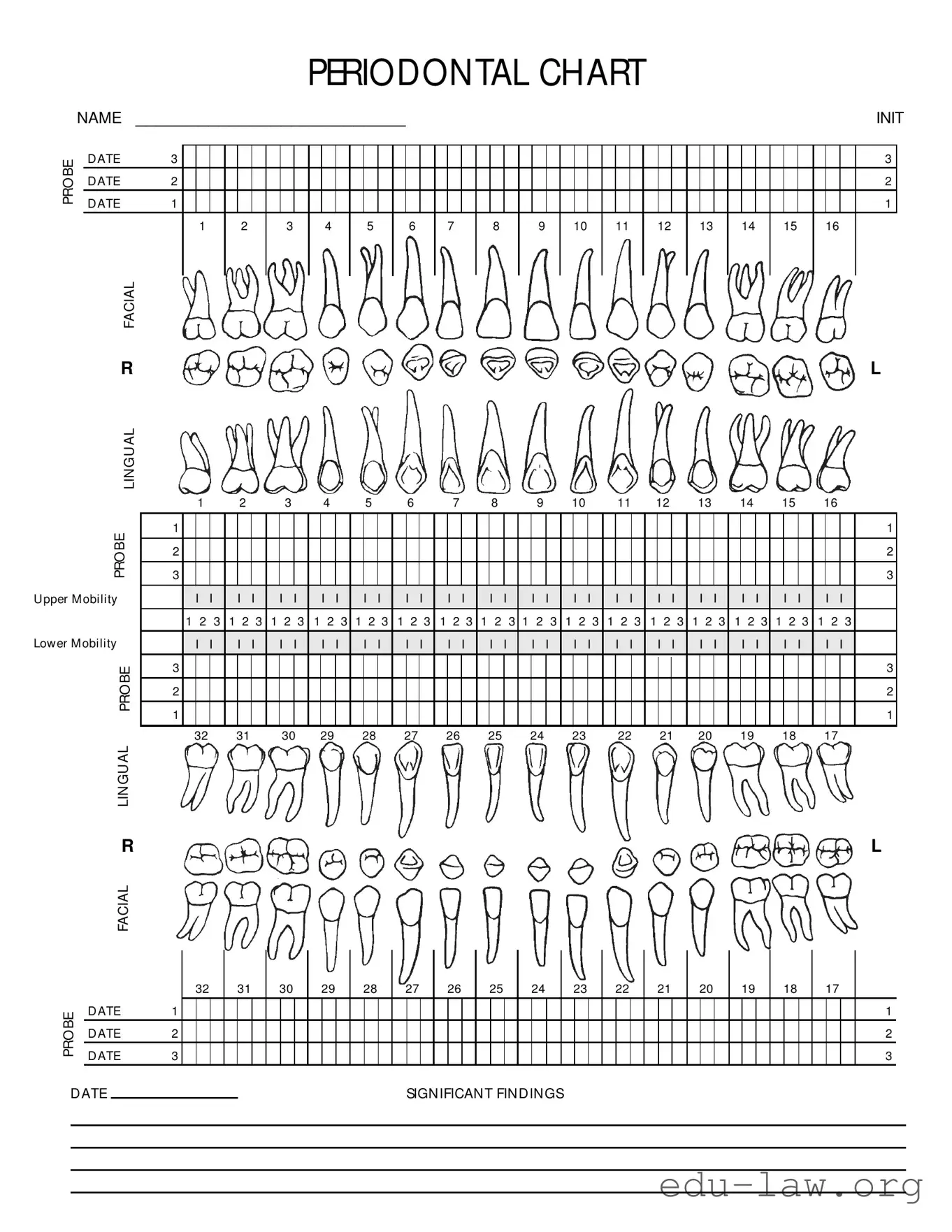
The Perio Chart form is an essential tool for dental professionals, providing a comprehensive overview of a patient's periodontal health. Each section of the form is meticulously designed to capture critical information, ensuring that no detail is overlooked during assessments. Starting with the patient's name and file number, the chart sets the stage for personalized care. It includes various diagnostic elements such as Clinical Attachment Loss (CAL), Bleeding on Probing (BOP), Probing Depth (PD), and the presence of calculus (Calc) and plaque (PI). These metrics are crucial for determining the severity of periodontal disease and for planning appropriate treatment strategies. Additionally, the chart incorporates both facial and lingual evaluations, allowing for a thorough examination of the gingival margin (GM) and the cementoenamel junction (CEJ). The inclusion of mobility assessments further aids in diagnosing the stability of teeth. This structured approach not only facilitates effective communication among dental team members but also enhances patient care through ongoing monitoring and re-evaluation during recall maintenance visits.
PERIODONTAL CHART
|
NAME |
__________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INIT |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BE |
|
D ATE |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
D ATE |
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
||
PRO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
D ATE |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
|
|
|||||||||||||||||
|
|
FACIAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
LIN GU AL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BE |
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
PRO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U pper M obility |
|
|
|
I |
I |
|
I |
I |
|
I I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
|
||||
|
|
|
|
|
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
1 2 3 |
|
|
||||||||||||||||||||||||||||||||
Low er M obility |
|
|
|
I |
I |
|
I |
I |
|
I I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
I |
I |
|
|
||||
|
|
BE |
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRO |
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32 |
|
31 |
|
30 |
29 |
|
28 |
|
27 |
|
26 |
|
25 |
|
24 |
|
23 |
|
22 |
|
21 |
20 |
|
19 |
|
18 |
|
17 |
|
|
|
||||||||||||||||||||
|
|
LIN GU AL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
FACIAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRO BE
|
|
|
32 |
|
31 |
|
30 |
|
29 |
|
28 |
|
27 |
|
26 |
|
25 |
|
24 |
|
23 |
|
22 |
|
21 |
|
20 |
|
19 |
|
18 |
|
17 |
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D ATE |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D ATE |
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
D ATE |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
D ATE |
|
SIGN IFICAN T FIN D IN GS |
|
|
|
|
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Patient Information | The form requires the patient's name, file number, and date of the examination. |
| Purpose | This chart is used to document periodontal health and treatment needs. |
| Diagnosis Fields | It includes sections for various diagnoses such as Clinical Attachment Loss (CAL) and Probing Depth (PD). |
| Measurement Indicators | Key indicators like Bleeding on Probing (BOP) and Plaque Index (PI) are included to assess periodontal health. |
| Mobility Assessment | The chart allows for recording the mobility of teeth, which can indicate periodontal issues. |
| Governing Law | In some states, the use of periodontal charts is governed by dental practice acts and regulations. |
| Signature Requirement | A supervisor's signature is required to validate the chart and the findings documented. |
| Clinical Terms | Abbreviations like GM (Gingival Margin) and CEJ (Cementoenamel Junction) are used for clarity. |
| Recall Maintenance | The form is also used for scheduling recall appointments to monitor periodontal health over time. |
Filling out the Perio Chart form is an important step in documenting a patient's periodontal health. This form helps track various indicators of gum health over time, allowing for better treatment planning and patient care. Follow these steps to accurately complete the form.
What is a Perio Chart form and why is it important?
The Perio Chart form is a crucial document used by dental professionals to assess and record the periodontal health of a patient. This chart provides a comprehensive overview of various factors, such as gum health, attachment levels, and the presence of plaque or calculus. It helps in diagnosing periodontal diseases and determining the appropriate treatment plan. Regular use of this form ensures that any changes in a patient's periodontal status are documented and monitored over time, which is essential for effective dental care.
What information is included in the Perio Chart form?
The Perio Chart form includes vital patient information such as the patient's name, file number, and date of the assessment. It also contains various diagnostic indicators like Clinical Attachment Loss (CAL), Bleeding on Probing (BOP), Probing Depth (PD), Plaque Index (PI), and Calculus (Calc). Additionally, the chart records the status of the Gingival Margin (GM) and any mobility of teeth, allowing for a thorough evaluation of periodontal health.
How is the data collected on the Perio Chart form?
Data collection on the Perio Chart form typically involves a dental professional conducting a clinical examination of the patient's gums and teeth. During this examination, the professional will measure probing depths, assess bleeding upon probing, and check for plaque and calculus. Each of these indicators is recorded in specific sections of the chart, providing a clear and organized way to track the patient's periodontal condition over time.
How often should the Perio Chart form be updated?
Updating the Perio Chart form is essential for maintaining accurate records of a patient's periodontal health. It is generally recommended that this form be updated at each dental visit, particularly during recall maintenance appointments or re-evaluations. Regular updates allow dental professionals to monitor any changes in the patient's condition and adjust treatment plans as necessary, ensuring optimal care.
What do the abbreviations on the Perio Chart form mean?
The Perio Chart form includes several abbreviations that represent different periodontal conditions. For example, CAL stands for Clinical Attachment Loss, which indicates the loss of support around the teeth. BOP refers to Bleeding on Probing, which signifies inflammation in the gums. PD stands for Probing Depth, measuring the depth of the gum pockets. Other abbreviations include PI for Plaque Index, Calc for Calculus, and GM for Gingival Margin. Understanding these terms is important for interpreting the chart accurately.
Who reviews and signs the Perio Chart form?
Typically, a qualified dental professional, such as a dentist or a dental hygienist, reviews and signs the Perio Chart form. Their signature indicates that they have assessed the patient's periodontal health and agree with the findings recorded on the chart. This review process is essential for ensuring that the patient receives appropriate care based on accurate and comprehensive evaluations.
Failing to complete the patient name and file number sections. These are essential for accurate record-keeping.
Not indicating the date of the evaluation. This can lead to confusion about the timing of treatments.
Overlooking the diagnosis section. Properly documenting the diagnosis is crucial for future reference.
Inaccurately marking CAL, BOP, PD, PI, Calc, and Mobility values. Ensure these measurements are precise to avoid misdiagnosis.
Not using the correct symbols for plaque and calculus. Remember to put an asterisk (*) if these are present.
Forgetting to note bleeding on probing with red. This is an important indicator of periodontal health.
Neglecting to fill out the Supervisor’s Signature section. This is necessary for validation of the chart.
Not reviewing the form for completeness before submission. A final check can prevent errors and ensure all necessary information is included.
The Perio Chart form is a crucial document in periodontal assessments, but it often accompanies several other forms and documents that enhance patient care and record-keeping. Below is a list of commonly used documents that work in conjunction with the Perio Chart form. Each plays a significant role in ensuring comprehensive patient management.
These documents collectively support the periodontal treatment process, ensuring that all aspects of patient care are meticulously documented and managed. It is crucial to maintain organized records for optimal patient outcomes and compliance with regulatory standards.
The Perio Chart form is similar to the Dental Exam form, which is often used during routine dental check-ups. Both documents aim to assess the health of a patient’s teeth and gums. The Dental Exam form typically includes sections for documenting the condition of each tooth, any existing restorations, and overall oral hygiene. Like the Perio Chart, it provides a systematic way for dental professionals to identify potential issues and track changes over time, ensuring that patients receive appropriate care.
Another related document is the Treatment Plan form. This form outlines the recommended procedures based on the findings from the Perio Chart and other assessments. It details the necessary treatments, their objectives, and timelines. Both forms are integral to patient care, as the Treatment Plan relies on the data collected in the Perio Chart to develop a comprehensive strategy for addressing periodontal health and improving the patient's overall oral condition.
The Progress Notes form serves as a record of ongoing treatment and patient interactions. It captures details about each visit, including observations made during examinations and any changes in the patient’s condition. Similar to the Perio Chart, the Progress Notes document specific findings, allowing dental professionals to monitor the effectiveness of treatments over time and adjust care as needed.
The Medical History form is another important document that shares similarities with the Perio Chart. This form collects vital information about a patient’s overall health, including any medical conditions or medications that may affect dental treatment. Understanding a patient’s medical history is crucial for interpreting the results on the Perio Chart and ensuring that any periodontal treatment is safe and effective.
The Oral Hygiene Assessment form is closely related to the Perio Chart as it evaluates a patient’s oral care habits. This document often includes questions about brushing, flossing, and other hygiene practices. Both forms aim to identify areas where patients may need additional education or support, helping to improve their periodontal health and prevent further issues.
The Radiographic Evaluation form complements the Perio Chart by providing visual insights into the patient’s dental health. This document includes findings from X-rays, which can reveal bone loss or other underlying issues not visible during a physical examination. Together with the Perio Chart, the Radiographic Evaluation helps create a complete picture of the patient’s periodontal status.
Lastly, the Referral Form may be used when a patient needs specialized care. This document outlines the reasons for the referral and includes relevant findings from the Perio Chart. Both forms ensure that the patient receives comprehensive care by facilitating communication between general dentists and specialists, such as periodontists, who can address more complex periodontal issues.
When filling out the Perio Chart form, it is essential to follow certain guidelines to ensure accuracy and clarity. Below is a list of things you should and shouldn't do.
Misconceptions about the Perio Chart form can lead to misunderstandings regarding its purpose and usage. Here are seven common misconceptions:
When filling out and using the Perio Chart form, there are several important points to keep in mind. Understanding these key takeaways can help ensure that the information is accurately recorded and effectively utilized.
By following these key points, you can effectively fill out and utilize the Perio Chart form, contributing to better patient care and accurate record-keeping.