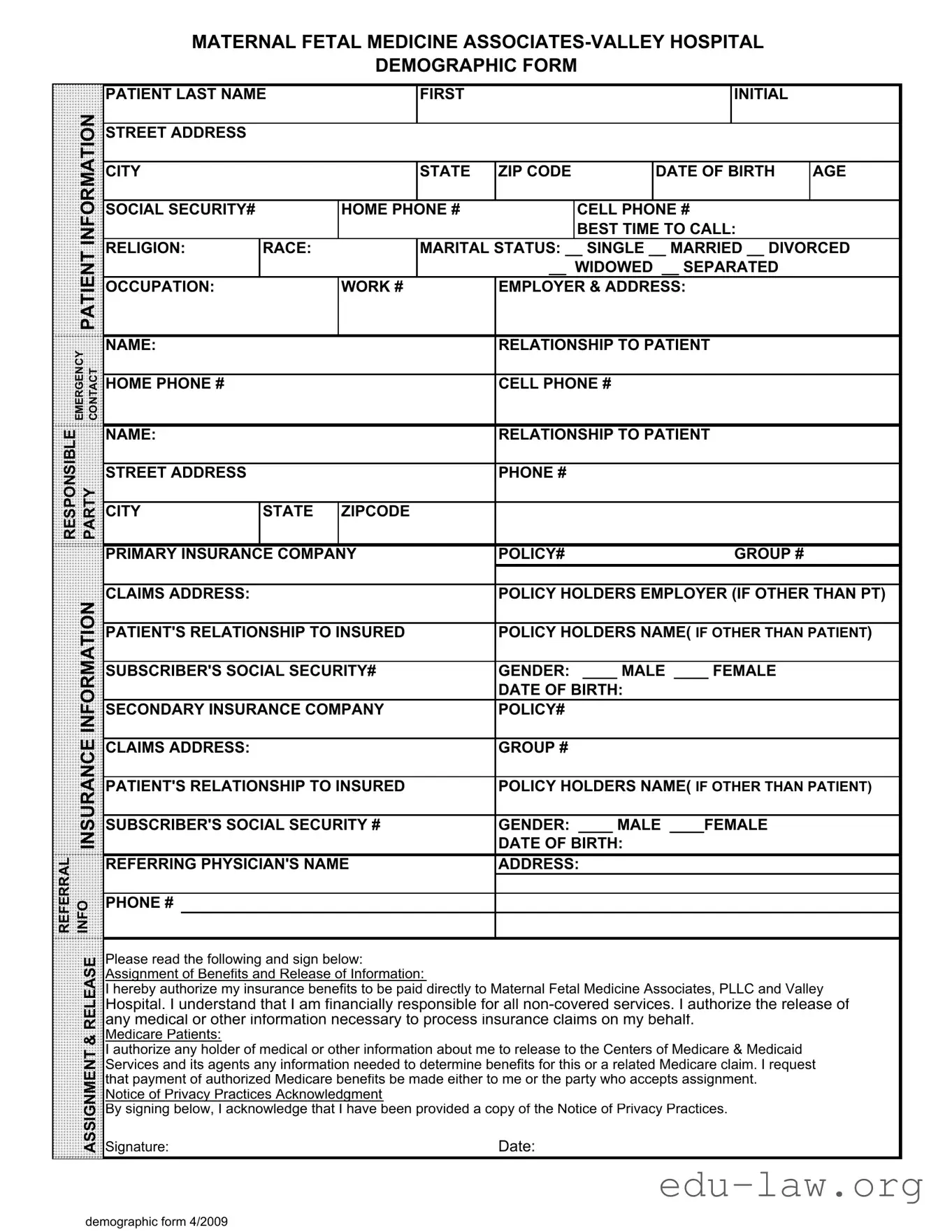
The Patient Demographics form is an essential document that collects vital information about patients seeking care, particularly in a maternal-fetal medicine setting. This form captures a variety of personal details, including the patient's name, address, date of birth, and contact numbers, ensuring that healthcare providers can reach patients effectively. Additionally, it gathers important demographic data such as marital status, occupation, and insurance information, which are crucial for billing and insurance claims. Emergency contact details are also included, allowing healthcare professionals to communicate with a designated person in case of urgent situations. Furthermore, the form addresses the patient's relationship to the insurance policyholder, which is important for verifying coverage and processing claims. By signing the form, patients authorize the release of their medical information necessary for insurance purposes and acknowledge their understanding of privacy practices. This comprehensive approach not only facilitates smooth interactions with healthcare providers but also supports effective management of patient care and insurance processes.
MATERNAL FETAL MEDICINE
DEMOGRAPHIC FORM
PATIENT LAST NAME |
FIRST |
INITIAL |
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
DATE OF BIRTH |
AGE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY# |
|
HOME PHONE # |
|
CELL PHONE # |
|
|||
|
|
|
|
|
|
|
|
BEST TIME TO CALL: |
|
|
|
PATIENT |
RELIGION: |
RACE: |
|
MARITAL STATUS: __ SINGLE __ MARRIED __ DIVORCED |
|||||
|
|
|
|
|
|
__ WIDOWED __ SEPARATED |
|
|||
|
|
|
|
|
|
|
|
|||
|
|
OCCUPATION: |
|
WORK # |
EMPLOYER & ADDRESS: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
EMERGENCY CONTACT |
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
||||
|
|
|
|
|
|
|
|
|
||
HOME PHONE # |
|
|
|
CELL PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||
RESPONSIBLE |
|
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
|||
PARTY |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIPCODE |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE COMPANY |
POLICY# |
GROUP # |
|
|||||
|
|
|
|
|
|
|
|
|||
|
INFORMATION |
CLAIMS ADDRESS: |
|
|
|
POLICY HOLDERS EMPLOYER (IF OTHER THAN PT) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
||||||||
|
|
|||||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY# |
GENDER: ____ MALE ____ FEMALE |
|
||||||
|
|
|
|
|
|
|
DATE OF BIRTH: |
|
|
|
|
|
SECONDARY INSURANCE COMPANY |
POLICY# |
|
|
|||||
|
INSURANCE |
|
|
|
|
|
|
|
|
|
|
CLAIMS ADDRESS: |
|
|
|
DATE OF BIRTH: |
|
|
|||
|
|
|
|
|
GROUP # |
|
|
|||
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
|||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY # |
GENDER: ____ MALE ____FEMALE |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
REFERRAL |
INFO |
REFERRING PHYSICIAN'S NAME |
ADDRESS: |
|
|
|||||
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELEASE |
Please read the following and sign below: |
|
|
|
|
||||
|
Assignment of Benefits and Release of Information: |
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
I hereby authorize my insurance benefits to be paid directly to Maternal Fetal Medicine Associates, PLLC and Valley |
||||||||
|
|
Hospital. I understand that I am financially responsible for all |
||||||||
|
|
any medical or other information necessary to process insurance claims on my behalf. |
|
|||||||
|
& |
Medicare Patients: |
|
|
|
|
|
|
|
|
|
I authorize any holder of medical or other information about me to release to the Centers of Medicare & Medicaid |
|
||||||||
|
ASSIGNMENT |
|
||||||||
|
Signature: |
|
|
|
Date: |
|
|
|||
|
|
Services and its agents any information needed to determine benefits for this or a related Medicare claim. I request |
||||||||
|
|
that payment of authorized Medicare benefits be made either to me or the party who accepts assignment. |
|
|||||||
|
|
Notice of Privacy Practices Acknowledgment |
|
|
|
|
||||
|
|
By signing below, I acknowledge that I have been provided a copy of the Notice of Privacy Practices. |
|
|||||||
demographic form 4/2009
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Patient Demographics form collects essential information about patients to ensure accurate medical records and facilitate billing processes. |
| Required Information | Patients must provide personal details such as name, address, date of birth, and insurance information. This data is crucial for effective communication and service delivery. |
| Emergency Contact | The form requires patients to list an emergency contact, including their relationship to the patient. This ensures that healthcare providers can reach someone in case of an emergency. |
| Insurance Information | Patients must provide details about their primary and secondary insurance policies, including policy numbers and claims addresses, to facilitate billing and claims processing. |
| Governing Laws | In the state of New Jersey, the use of Patient Demographics forms is governed by the New Jersey Statutes Annotated § 26:2H-12.4, which ensures patient privacy and data protection. |
Completing the Patient Demographics form is an essential step in ensuring that your medical information is accurately recorded. This information will be used to facilitate your care and manage your insurance claims effectively.
What is the purpose of the Patient Demographics form?
The Patient Demographics form collects essential information about patients, including personal details, insurance information, and emergency contacts. This data helps healthcare providers deliver appropriate care and ensures efficient processing of insurance claims.
What information do I need to provide on the form?
You will need to provide your full name, address, date of birth, social security number, contact numbers, marital status, occupation, and insurance details. Additionally, emergency contact information and the responsible party's details are required.
Why is my Social Security number required?
Your Social Security number is used primarily for identification purposes. It helps in verifying your identity and is often necessary for insurance billing and claims processing.
How is my personal information protected?
Your personal information is treated with the utmost confidentiality. The healthcare provider is required to comply with privacy regulations, ensuring that your data is securely stored and only shared with authorized personnel for medical and billing purposes.
What should I do if I do not have insurance?
If you do not have insurance, you can indicate this on the form. The healthcare provider will discuss payment options and any financial assistance programs that may be available to you.
Can I update my information after submitting the form?
Yes, you can update your information at any time. If there are changes to your contact details, insurance, or other relevant information, inform the office staff during your next visit or contact them directly.
What happens if I don’t complete the form?
Failure to complete the form may delay your appointment or treatment. It is crucial to provide accurate and complete information to ensure a smooth process for both you and the healthcare provider.
Do I need to sign the release section of the form?
Yes, signing the release section is important. It authorizes your insurance benefits to be paid directly to the healthcare provider and allows them to release necessary medical information to process your claims. Without your signature, claims may not be processed efficiently.
Incomplete Information: Failing to fill out all required fields can lead to delays in processing. Ensure that every section, especially personal details like name and date of birth, is complete.
Incorrect Contact Information: Providing wrong phone numbers or addresses can hinder communication. Double-check that all contact details are accurate and up-to-date.
Missing Insurance Details: Omitting information about insurance providers can complicate billing. Include both primary and secondary insurance details, if applicable.
Neglecting Emergency Contacts: Forgetting to list an emergency contact can be problematic. Always provide a reliable person’s name and phone number for emergencies.
Inaccurate Relationship Information: Misstating relationships can lead to confusion. Clearly indicate the relationship of emergency contacts and responsible parties to the patient.
Overlooking Signature Requirements: Not signing the form can render it invalid. Make sure to sign and date the document where indicated to confirm your consent.
The Patient Demographics form is a crucial document for collecting essential information about patients. Alongside this form, several other documents are commonly utilized to ensure comprehensive patient care and accurate processing of information. Below is a list of these documents, along with brief descriptions of their purposes.
These documents work together with the Patient Demographics form to create a complete picture of the patient's health and insurance status. Proper completion and management of these forms are vital for efficient healthcare delivery and administrative processes.
The Patient Registration Form is similar to the Patient Demographics form in that it collects essential information about a patient before their first visit. This form typically includes the patient's name, contact information, and insurance details, much like the Demographics form. Both documents aim to create a comprehensive profile that helps healthcare providers understand their patients better and ensures that billing and communication processes run smoothly.
The Medical History Form serves a similar purpose by gathering detailed information about a patient's past health issues, surgeries, and medications. While the Patient Demographics form focuses on personal and contact information, the Medical History Form dives deeper into the patient's health background. This information is crucial for healthcare providers to offer tailored care and to avoid potential complications during treatment.
The Insurance Information Form also parallels the Patient Demographics form by specifically targeting the patient's insurance details. It collects information such as the insurance company name, policy number, and the relationship of the patient to the insured. Both forms work together to ensure that healthcare providers can efficiently process claims and understand the patient's coverage, which is vital for financial transparency in healthcare services.
The Emergency Contact Form is another document that shares similarities with the Patient Demographics form. It gathers information about who to contact in case of an emergency, including the contact's relationship to the patient and their phone numbers. While the Demographics form includes this information, the Emergency Contact Form focuses solely on ensuring that healthcare providers can reach someone quickly if the patient cannot communicate their needs.
The Consent for Treatment Form is akin to the Patient Demographics form in that it establishes a formal agreement between the patient and the healthcare provider. This document confirms that the patient understands and agrees to the proposed treatments and procedures. While the Demographics form collects information, the Consent for Treatment Form ensures that the patient is informed and consents to the care they will receive, establishing trust and clarity in the patient-provider relationship.
Lastly, the Financial Responsibility Agreement shares a connection with the Patient Demographics form by outlining the patient's obligations regarding payment for services rendered. This document ensures that the patient understands their financial responsibilities, similar to how the Demographics form collects insurance information. Both documents aim to clarify the financial aspects of healthcare, helping to prevent misunderstandings and ensuring that patients are aware of their obligations before receiving care.
When filling out the Patient Demographics form, it's important to be thorough and accurate. Here are some key things to keep in mind:
Following these guidelines will help ensure that your information is processed smoothly and efficiently. Take your time to review the form before submitting it, and don't hesitate to reach out if you have any questions.
In reality, completing the form is essential for accurate patient identification and insurance processing.
The form also gathers information about insurance, emergency contacts, and medical history, which are crucial for comprehensive care.
While most fields are important, some may be left blank if they do not apply to the patient.
Existing patients may need to update their information periodically, making the form relevant for all.
Providing accurate insurance details is vital for billing and coverage verification.
All data collected is protected under privacy laws and is handled with strict confidentiality.
It serves multiple purposes, including treatment planning and coordination of care.
Most patients find the form straightforward and quick to complete, taking only a few minutes.
When filling out the Patient Demographics form, it is essential to ensure accuracy and completeness. Here are some key takeaways to keep in mind: