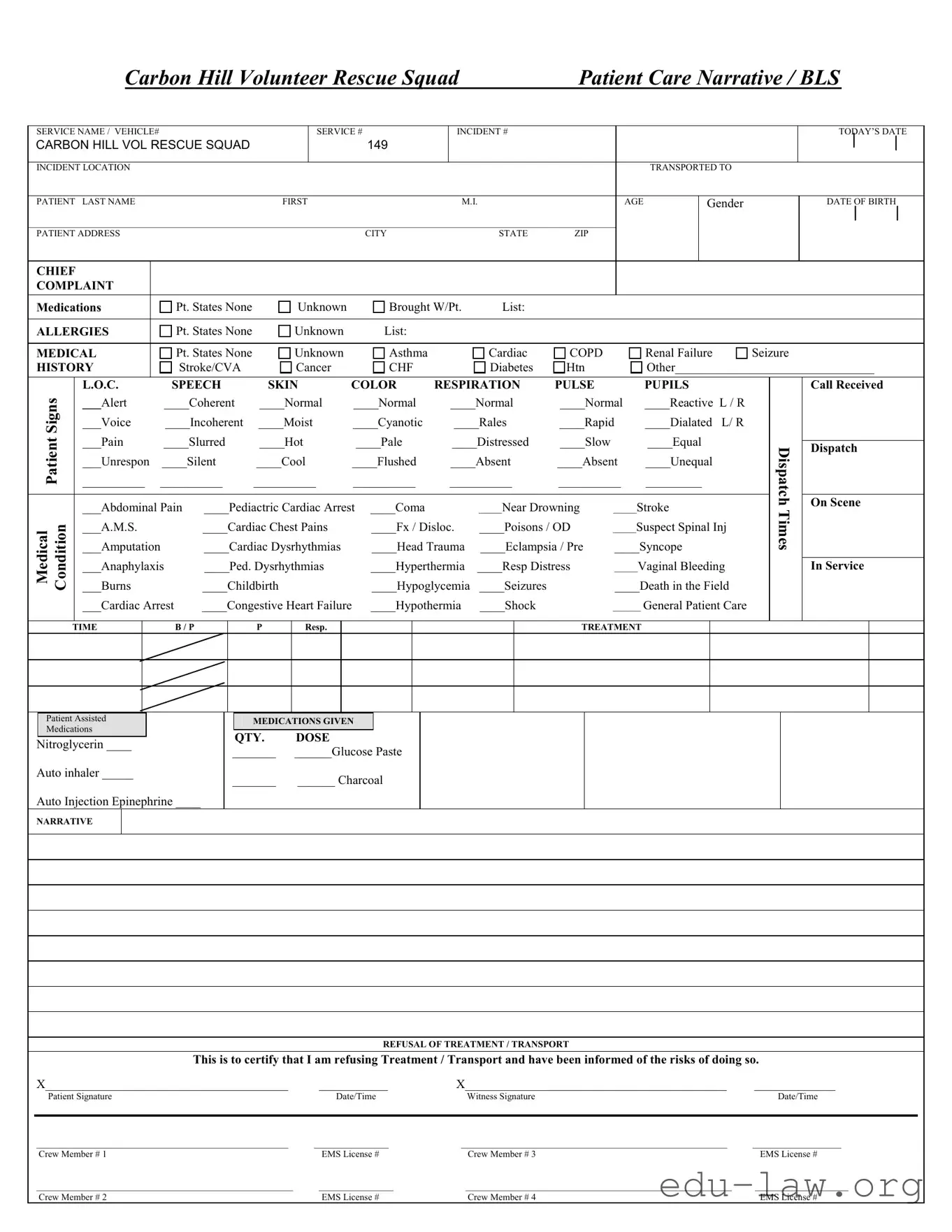
The Patient Care Report (PCR) form serves as a vital tool in documenting the care provided to patients during emergency medical situations. This comprehensive form captures essential details, beginning with the service name and incident specifics, including the date, location, and vehicle information. It records patient demographics, such as name, age, gender, and address, ensuring that responders have accurate information at hand. The chief complaint section allows for a clear identification of the patient's primary issue, while the medical history segment highlights any relevant conditions or allergies. Additionally, the form includes critical observations like level of consciousness, speech, skin color, respiration, pulse, and pupil response, which are essential for assessing the patient's condition. Treatment details are meticulously noted, including medications administered and any patient refusals for treatment or transport. The narrative section provides space for crew members to document their observations and actions taken during the incident. Overall, the PCR form is an indispensable component in delivering effective patient care and ensuring continuity of information for further medical treatment.
|
|
|
Carbon Hill Volunteer Rescue Squad |
|
Patient Care Narrative / BLS |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
SERVICE NAME / VEHICLE# |
|
|
|
SERVICE # |
|
INCIDENT # |
|
|
|
|
|
|
|
|
|
TODAY’S DATE |
||||||||
CARBON HILL VOL RESCUE SQUAD |
|
|
|
149 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INCIDENT LOCATION |
|
|
|
|
|
|
|
|
|
|
|
|
TRANSPORTED TO |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PATIENT |
LAST NAME |
|
|
FIRST |
|
|
|
M.I. |
|
|
AGE |
|
Gender |
|
|
|
|
DATE OF BIRTH |
||||||
______________________________________________________________________________________________________________________________ |
|
|
|
|
|
|
|
|
|
|||||||||||||||
PATIENT ADDRESS |
|
|
|
|
|
CITY |
|
|
STATE |
ZIP |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHIEF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLAINT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Medications |
|
Pt. States None |
Unknown |
|
Brought W/Pt. |
List: |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ALLERGIES |
|
Pt. States None |
Unknown |
|
List: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MEDICAL |
|
Pt. States None |
Unknown |
|
Asthma |
|
|
Cardiac |
COPD |
|
|
Renal Failure |
Seizure |
|
|
|
||||||||
HISTORY |
|
Stroke/CVA |
Cancer |
|
CHF |
|
|
Diabetes |
Htn |
|
|
Other________________________________ |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Signs |
|
L.O.C. |
SPEECH |
SKIN |
COLOR |
RESPIRATION |
PULSE |
|
|
PUPILS |
|
|
|
|
Call Received |
|||||||||
|
___Alert |
____Coherent |
____Normal |
____Normal |
|
____Normal |
____Normal |
____Reactive L / R |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
___Voice |
____Incoherent |
____Moist |
____Cyanotic |
|
____Rales |
____Rapid |
____Dialated L/ R |
|
|
|
|
|
|
|||||||||
Patient |
|
___Pain |
____Slurred |
____Hot |
|
____Pale |
|
____Distressed |
____Slow |
|
|
____Equal |
|
|
Dispatch |
|
On Scene |
|||||||
|
|
|
|
|
|
|
|
|
|
Dispatch |
||||||||||||||
|
|
___Unrespon |
____Silent |
____Cool |
____Flushed |
|
____Absent |
____Absent |
____Unequal |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
__________ __________ |
__________ |
__________ |
__________ |
__________ |
_________ |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___Abdominal Pain |
____Pediactric Cardiac Arrest |
____Coma |
|
|
_____Near Drowning |
_____Stroke |
|
|
Times |
|
|
|
||||||||||
Medical Condition |
|
___A.M.S. |
|
____Cardiac Chest Pains |
|
____Fx / Disloc. |
____Poisons / OD |
_____Suspect Spinal Inj |
|
|
|
|
|
|||||||||||
|
___Burns |
|
____Childbirth |
|
____Hypoglycemia |
____Seizures |
|
____Death in the Field |
|
|
|
|
|
|||||||||||
|
|
___Amputation |
|
____Cardiac Dysrhythmias |
|
____Head Trauma |
____Eclampsia / Pre |
____Syncope |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
___Anaphylaxis |
____Ped. Dysrhythmias |
|
____Hyperthermia |
____Resp Distress |
_____Vaginal Bleeding |
|
|
|
|
In Service |
||||||||||||
|
|
___Cardiac Arrest |
____Congestive Heart Failure |
____Hypothermia |
____Shock |
|
______ General Patient Care |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TIME
B / P
P
Resp.
TREATMENT
Patient Assisted
Medications
Nitroglycerin ____
Auto inhaler _____
Auto Injection Epinephrine ____
MEDICATIONS GIVEN
QTY. |
DOSE |
_______ |
______Glucose Paste |
_______ |
______ Charcoal |
NARRATIVE
REFUSAL OF TREATMENT / TRANSPORT
This is to certify that I am refusing Treatment / Transport and have been informed of the risks of doing so.
X_______________________________________ |
___________ |
X__________________________________________ |
_____________ |
Patient Signature |
Date/Time |
Witness Signature |
Date/Time |
|
|
|
|
______________________________________________________ |
________________ |
_________________________________________________________ |
___________________ |
Crew Member # 1 |
EMS License # |
Crew Member # 3 |
EMS License # |
_______________________________________________________ |
________________ |
_________________________________________________________ |
____________________ |
Crew Member # 2 |
EMS License # |
Crew Member # 4 |
EMS License # |
| Fact Name | Detail |
|---|---|
| Form Purpose | The Patient Care Report (PCR) form is used to document the medical care provided to patients during emergency medical services. |
| Patient Identification | Essential patient information includes the patient's last name, first name, middle initial, age, gender, and date of birth. |
| Chief Complaint | The form requires the documentation of the chief complaint, which is the primary reason for the patient's medical attention. |
| Medical History | It includes a section to note the patient's medical history, listing conditions such as asthma, cardiac issues, and diabetes. |
| Vital Signs | Vital signs such as blood pressure, respiration rate, and pulse must be recorded to assess the patient's condition. |
| Treatment Provided | The form includes a section for documenting treatments administered, including medications given and their dosages. |
| Legal Compliance | In many states, the use of the PCR form is governed by laws pertaining to emergency medical services documentation, such as the Health Insurance Portability and Accountability Act (HIPAA). |
Completing the Patient Care Report form is essential for documenting patient interactions and ensuring accurate medical records. Follow these steps carefully to ensure all necessary information is captured accurately.
What is the purpose of the Patient Care Report form?
The Patient Care Report (PCR) form serves as a comprehensive record of the medical care provided to a patient during an emergency response. It documents essential information such as the patient's demographics, chief complaints, medical history, and the treatments administered. This form is crucial for ensuring continuity of care, as it provides healthcare providers with vital details when the patient is transferred to a hospital or another facility. Additionally, it serves as a legal document that can be referenced in case of disputes or investigations.
What information is required on the Patient Care Report form?
The form requires a variety of information to ensure accurate documentation. Key sections include the patient's name, age, gender, and date of birth, as well as their address and chief complaint. Medical history is also critical; responders must note any known allergies, existing medical conditions, and medications the patient is currently taking. Observations made during the assessment, such as vital signs and the patient's level of consciousness, should be recorded meticulously. This information not only aids in patient care but also helps in legal and billing processes.
What happens if a patient refuses treatment or transport?
If a patient refuses treatment or transport, the PCR form includes a specific section for documenting this decision. The patient must sign the form to acknowledge their refusal and confirm that they have been informed of the potential risks associated with not receiving care. This signature acts as a safeguard for both the patient and the emergency responders, ensuring that the patient understands their choice and that the responders have fulfilled their duty to inform. Proper documentation of such refusals is vital to protect against liability issues.
Who is responsible for completing the Patient Care Report form?
The responsibility of completing the Patient Care Report typically falls on the crew members who provided care during the incident. Each crew member involved in the patient's care should contribute to the report, ensuring that all relevant details are captured accurately. This collaborative approach helps create a comprehensive narrative of the patient’s condition and the interventions performed. Each crew member must sign the form, including their EMS license numbers, to validate the information recorded and to maintain accountability.
Neglecting to include patient demographics: Failing to fill out the patient’s last name, first name, age, gender, and date of birth can lead to confusion and miscommunication.
Inaccurate incident details: Omitting the incident location or service numbers can hinder proper documentation and follow-up.
Not documenting the chief complaint: Leaving this section blank or vague can result in inadequate understanding of the patient's condition.
Ignoring allergies: Failing to list known allergies can pose serious risks during treatment.
Incomplete medical history: Not providing a thorough medical history may lead to missed critical information affecting patient care.
Misreporting vital signs: Errors in recording vital signs can lead to improper assessment and treatment decisions.
Skipping the narrative section: Leaving out a detailed narrative can result in a lack of clarity about the patient’s condition and treatment provided.
Failure to document refusals: Not properly documenting a patient's refusal of treatment or transport can create legal issues.
Missing signatures: Omitting patient or witness signatures can invalidate the report and complicate legal matters.
Not double-checking for accuracy: Failing to review the report for errors before submission can lead to misunderstandings and complications in patient care.
The Patient Care Report (PCR) form is essential for documenting the care provided to patients during emergency medical situations. However, it is often accompanied by other important forms and documents that help ensure comprehensive patient care and proper record-keeping. Below is a list of some commonly used documents that may accompany the PCR.
These forms and documents work together to create a comprehensive record of patient care, ensuring that all aspects of treatment are documented and communicated effectively. Understanding each of these documents can enhance the quality of care provided and streamline the administrative process in emergency medical situations.
The Emergency Medical Services (EMS) Run Report is similar to the Patient Care Report form in that it documents the details of a medical incident. This report includes information such as the patient's demographics, the nature of the emergency, and the treatment provided. Just like the Patient Care Report, it serves to ensure continuity of care and provides critical information for future medical treatment.
The Incident Report is another document that shares similarities with the Patient Care Report. It captures the circumstances surrounding an emergency, including the time, location, and nature of the incident. While the Patient Care Report focuses more on patient care and treatment, the Incident Report highlights the overall context and response of emergency services, making both essential for comprehensive documentation.
The Medical History Form is a crucial document that resembles the Patient Care Report. It collects detailed information about a patient's past medical conditions, medications, and allergies. This form aids healthcare providers in understanding a patient's background, just as the Patient Care Report does during an emergency response.
The Consent for Treatment Form is also akin to the Patient Care Report. It requires patients to give permission for medical treatment, often including information about risks and benefits. This document is vital in ensuring that patients are informed, paralleling the Patient Care Report's emphasis on patient rights and informed consent.
The Transfer of Care Form is similar in purpose to the Patient Care Report, as it documents the handoff of a patient from one healthcare provider to another. This form ensures that all relevant information about the patient's condition and treatment is communicated effectively, just like the detailed accounts found in the Patient Care Report.
The Discharge Summary is another related document. It provides a comprehensive overview of a patient's treatment and condition at the time of discharge from a healthcare facility. Like the Patient Care Report, it includes critical information that can influence future care and treatment decisions.
The Trauma Assessment Form is closely related to the Patient Care Report, especially in emergency situations. It focuses specifically on trauma patients, documenting injuries, vital signs, and treatment provided. Both forms aim to ensure that healthcare providers have the necessary information to deliver appropriate care.
The Patient Transport Record is similar as it tracks the details of a patient during transport. This document includes information about the patient's condition, vital signs, and care provided en route to a medical facility. Like the Patient Care Report, it emphasizes the importance of continuous monitoring and documentation.
The Prescription Record is another document that shares similarities with the Patient Care Report. It details the medications prescribed to a patient, including dosages and instructions. This record is essential for ensuring that patients receive the correct medications, paralleling the Patient Care Report's focus on medication administration during emergencies.
Finally, the Follow-Up Care Plan is akin to the Patient Care Report in that it outlines the next steps in a patient's treatment after an emergency. This document includes recommendations for further care and monitoring, ensuring that patients receive ongoing support, much like the information recorded in the Patient Care Report.
When filling out the Patient Care Report form, attention to detail is crucial. Here’s a list of dos and don'ts to ensure accuracy and completeness.
Misconceptions about the Patient Care Report (PCR) form can lead to misunderstandings regarding its purpose and importance. Here are nine common misconceptions:
Understanding these misconceptions can help ensure that the Patient Care Report form is used effectively and appropriately.
When filling out and utilizing the Patient Care Report (PCR) form, attention to detail and accuracy are paramount. Here are some key takeaways to consider:
By following these guidelines, the Patient Care Report can serve as a vital tool in providing quality care and maintaining accurate medical records.