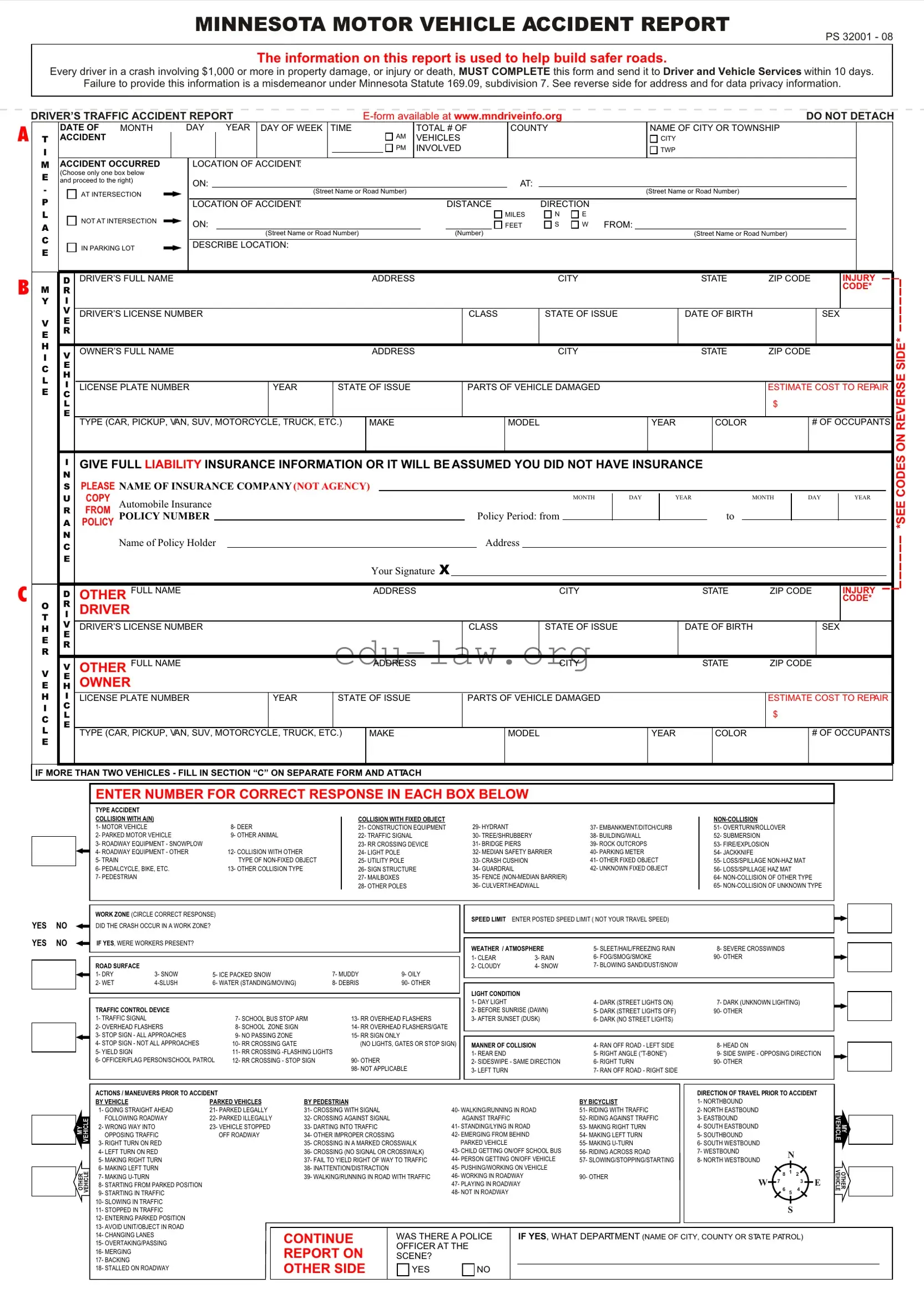
The Minnesota Accident Report form is a crucial document that every driver must complete after being involved in a motor vehicle accident, especially if the incident results in property damage exceeding $1,000 or involves injury or death. This form serves multiple purposes, including aiding in the collection of data to enhance road safety across the state. It requires essential information such as the date, time, and location of the accident, as well as details about the vehicles and individuals involved. Drivers must provide their personal information, including name, address, and driver's license number, alongside their insurance details. The form also prompts users to describe the accident's circumstances and the type of collision that occurred. Additionally, it includes sections for documenting weather conditions, traffic control devices, and any injuries sustained. Timeliness is critical; the report must be submitted to Driver and Vehicle Services within ten days of the accident. Failing to do so may result in legal penalties. Understanding how to accurately fill out this form is vital for drivers to ensure compliance with Minnesota law and to contribute to safer roadways.
MINNESOTA MOTOR VEHICLE ACCIDENT REPORT
PS 32001 - 08
The information on this report is used to help build safer roads.
Every driver in a crash involving $1,000 or more in property damage, or injury or death, MUST COMPLETE this form and send it to Driver and Vehicle Services within 10 days.
Failure to provide this information is a misdemeanor under Minnesota Statute 169.09, subdivision 7. See reverse side for address and for data privacy information.
A
B
C
DRIVER’S TRAFFIC ACCIDENT REPORT |
|
|
|
DO NOT DETACH |
|||||||||||||||||||||||||
|
|
DATE OF |
MONTH |
DAY |
YEAR |
DAY OF WEEK |
TIME |
|
|
TOTAL # OF |
|
COUNTY |
|
|
NAME OF CITY OR TOWNSHIP |
|
|
|
|
||||||||||
T |
|
ACCIDENT |
|
|
|
|
|
|
|
|
|
|
AM |
VEHICLES |
|
|
|
|
|
CITY |
|
|
|
|
|
||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
INVOLVED |
|
|
|
|
|
TWP |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
M |
|
ACCIDENT OCCURRED |
LOCATION OF ACCIDENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
(Choose only one box below |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
and proceed to the right) |
ON: |
|
|
|
|
|
|
|
|
|
|
|
|
|
AT: |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
AT INTERSECTION |
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
P |
|
|
|
|
|
LOCATION OF ACCIDENT: |
|
|
|
|
DISTANCE |
|
|
DIRECTION |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILES |
N |
E |
|
|
|
|
|
|
|
|
A |
|
|
NOT AT INTERSECTION |
ON: |
|
|
|
|
|
|
|
|
|
|
FEET |
S |
W FROM: |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
C |
|
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
(Number) |
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
||||
|
|
IN PARKING LOT |
DESCRIBE LOCATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
D DRIVER’S FULL NAME |
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
INJURY |
||||||
M |
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
|
|
CLASS |
|
|
STATE OF ISSUE |
|
DATE OF BIRTH |
|
SEX |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
VE
E R
H |
V |
|
OWNER’S FULL NAME |
|
|
ADDRESS |
|
CITY |
|
STATE |
ZIP CODE |
||
I |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
E |
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE PLATE NUMBER |
YEAR |
STATE OF ISSUE |
PARTS OF VEHICLE DAMAGED |
|
|
|
ESTIMATE COST TO REPAIR |
||||
E |
C |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
$ |
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
MODEL |
YEAR |
|
COLOR |
|
# OF OCCUPANTS |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IGIVE FULL LIABILITY INSURANCE INFORMATION OR IT WILL BE ASSUMED YOU DID NOT HAVE INSURANCE
N
SPLEASE NAME OF INSURANCE COMPANY (NOT AGENCY)
|
|
U |
COPY |
Automobile Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
YEAR |
|
|
|
MONTH |
|
DAY |
|
YEAR |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
R |
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
POLICY NUMBER |
|
|
|
|
|
|
|
|
Policy Period: from |
|
|
|
|
|
|
|
|
to |
|
|
|
|
|
|
|
|
|||||||
|
|
A |
POLICY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
Name of Policy Holder |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your Signature X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
D |
OTHER |
FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||||
O |
|
R |
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
CLASS |
|
STATE OF ISSUE |
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|||||||||||||||
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
V |
OTHER FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|||||||||||||
|
HE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
OWNER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
H |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
LICENSE PLATE NUMBER |
|
YEAR |
STATE OF ISSUE |
|
PARTS OF VEHICLE DAMAGED |
|
|
|
|
|
|
|
|
ESTIMATE COST TO REPAIR |
||||||||||||||||||||
I |
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
C |
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
|
MODEL |
|
|
|
|
YEAR |
|
|
COLOR |
|
|
# OF OCCUPANTS |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
IF MORE THAN TWO VEHICLES - FILL IN SECTION “C” ON SEPARATE FORM AND ATTACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*SEE CODES ON REVERSE SIDE*
ENTER NUMBER FOR CORRECT RESPONSE IN EACH BOX BELOW
|
|
|
|
TYPE ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COLLISION WITH A(N) |
|
|
|
|
COLLISION WITH FIXED OBJECT |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
1- MOTOR VEHICLE |
|
|
8- DEER |
|
21- CONSTRUCTION EQUIPMENT |
29- HYDRANT |
|
37- EMBANKMENT/DITCH/CURB |
51- OVERTURN/ROLLOVER |
|
|
|
|
|
2- PARKED MOTOR VEHICLE |
|
9- OTHER ANIMAL |
|
22- TRAFFIC SIGNAL |
30- TREE/SHRUBBERY |
|
38- BUILDING/WALL |
52- SUBMERSION |
||
|
|
|
|
3- ROADWAY EQUIPMENT - SNOWPLOW |
|
|
|
23- RR CROSSING DEVICE |
31- BRIDGE PIERS |
|
39- ROCK OUTCROPS |
53- FIRE/EXPLOSION |
||
|
|
|
|
4- ROADWAY EQUIPMENT - OTHER |
|
12- COLLISION WITH OTHER |
|
24- LIGHT POLE |
|
32- MEDIAN SAFETY BARRIER |
40- PARKING METER |
54- JACKKNIFE |
||
|
|
|
|
5- TRAIN |
|
|
TYPE OF |
|
25- UTILITY POLE |
33- CRASH CUSHION |
|
41- OTHER FIXED OBJECT |
55- LOSS/SPILLAGE |
|
|
|
|
|
6- PEDALCYCLE, BIKE, ETC. |
|
13- OTHER COLLISION TYPE |
|
26- SIGN STRUCTURE |
34- GUARDRAIL |
|
42- UNKNOWN FIXED OBJECT |
56- LOSS/SPILLAGE HAZ MAT |
||
|
|
|
|
7- PEDESTRIAN |
|
|
|
|
27- MAILBOXES |
|
35- FENCE |
|
64- |
|
|
|
|
|
|
|
|
|
|
28- OTHER POLES |
36- CULVERT/HEADWALL |
|
65- |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
WORK ZONE (CIRCLE CORRECT RESPONSE) |
|
|
|
|
SPEED LIMIT ENTER POSTED SPEED LIMIT ( NOT YOUR TRAVEL SPEED) |
|
||||
YES |
NO |
|
|
|
|
|
|
|
|
|||||
DID THE CRASH OCCUR IN A WORK ZONE? |
|
|
|
|
|
|
|
|
|
|||||
YES |
NO |
IF YES, WERE WORKERS PRESENT? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
WEATHER / ATMOSPHERE |
5- SLEET/HAIL/FREEZING RAIN |
8- SEVERE CROSSWINDS |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
1- CLEAR |
3- RAIN |
6- FOG/SMOG/SMOKE |
90- OTHER |
|
|
|
|
ROAD SURFACE |
|
|
|
|
|
|
2- CLOUDY |
4- SNOW |
7- BLOWING SAND/DUST/SNOW |
|
|
|
|
|
1- DRY |
3- SNOW |
5- ICE PACKED SNOW |
7- MUDDY |
9- OILY |
|
|
|
|
||
|
|
|
|
2- WET |
6- WATER (STANDING/MOVING) |
8- DEBRIS |
90- OTHER |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIGHT CONDITION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1- DAY LIGHT |
|
4- DARK (STREET LIGHTS ON) |
7- DARK (UNKNOWN LIGHTING) |
|
|
|
|
TRAFFIC CONTROL DEVICE |
|
|
|
|
|
2- BEFORE SUNRISE (DAWN) |
5- DARK (STREET LIGHTS OFF) |
90- OTHER |
||
|
|
|
|
1- TRAFFIC SIGNAL |
|
|
7- SCHOOL BUS STOP ARM |
|
13- RR OVERHEAD FLASHERS |
3- AFTER SUNSET (DUSK) |
6- DARK (NO STREET LIGHTS) |
|
||
|
|
|
|
2- OVERHEAD FLASHERS |
|
8- SCHOOL ZONE SIGN |
|
14- RR OVERHEAD FLASHERS/GATE |
|
|
|
|
||
|
|
|
|
3- STOP SIGN - ALL APPROACHES |
|
9- NO PASSING ZONE |
|
15- RR SIGN ONLY |
|
|
|
|
|
|
|
|
|
|
4- STOP SIGN - NOT ALL APPROACHES |
|
10- RR CROSSING GATE |
|
(NO LIGHTS, GATES OR STOP SIGN) |
MANNER OF COLLISION |
4- RAN OFF ROAD - LEFT SIDE |
8- HEAD ON |
|||
|
|
|
|
5- YIELD SIGN |
|
|
11- RR CROSSING |
|
1- REAR END |
|
5- RIGHT ANGLE |
9- SIDE SWIPE - OPPOSING DIRECTION |
||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
6- OFFICER/FLAG PERSON/SCHOOL PATROL |
12- RR CROSSING - STOP SIGN |
|
90- OTHER |
|
2- SIDESWIPE - SAME DIRECTION |
6- RIGHT TURN |
90- OTHER |
|||
|
|
|
|
|
|
|
|
|
98- NOT APPLICABLE |
3- LEFT TURN |
|
7- RAN OFF ROAD - RIGHT SIDE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MY |
VEHICLE |
OTHER |
VEHICLE |
ACTIONS / MANEUVERS PRIOR TO ACCIDENT
BY VEHICLE |
PARKED VEHICLES |
1- GOING STRAIGHT AHEAD |
21- PARKED LEGALLY |
FOLLOWING ROADWAY |
22- PARKED ILLEGALLY |
2- WRONG WAY INTO |
23- VEHICLE STOPPED |
OPPOSING TRAFFIC |
OFF ROADWAY |
3- RIGHT TURN ON RED |
|
4- LEFT TURN ON RED |
|
5- MAKING RIGHT TURN |
|
6- MAKING LEFT TURN |
|
7- MAKING |
|
8- STARTING FROM PARKED POSITION |
|
9- STARTING IN TRAFFIC |
|
10- SLOWING IN TRAFFIC |
|
11- STOPPED IN TRAFFIC |
|
12- ENTERING PARKED POSITION |
|
13- AVOID UNIT/OBJECT IN ROAD |
|
14- CHANGING LANES |
|
15- OVERTAKING/PASSING |
|
16- MERGING |
|
17- BACKING |
|
18- STALLED ON ROADWAY |
|
|
|
|
|
|
|
|
|
|
DIRECTION OF TRAVEL PRIOR TO ACCIDENT |
|||||||
BY PEDESTRIAN |
|
|
|
|
BY BICYCLIST |
1- NORTHBOUND |
|
|
|
|
|
|
|
|
31- CROSSING WITH SIGNAL |
|
40- WALKING/RUNNING IN ROAD |
51- RIDING WITH TRAFFIC |
2- NORTH EASTBOUND |
|
|
|
|
|
|
|
|||
32- CROSSING AGAINST SIGNAL |
|
AGAINST TRAFFIC |
|
52- RIDING AGAINST TRAFFIC |
3- EASTBOUND |
|
|
|
|
|
|
|
||
33- DARTING INTO TRAFFIC |
|
41- STANDING/LYING IN ROAD |
53- MAKING RIGHT TURN |
4- SOUTH EASTBOUND |
|
|
|
|
|
|
|
|||
34- OTHER IMPROPER CROSSING |
|
42- EMERGING FROM BEHIND |
54- MAKING LEFT TURN |
5- SOUTHBOUND |
|
|
|
|
|
|
|
|||
35- CROSSING IN A MARKED CROSSWALK |
PARKED VEHICLE |
|
55- MAKING |
6- SOUTH WESTBOUND |
|
|
|
|
|
|
|
|||
36- CROSSING (NO SIGNAL OR CROSSWALK) |
43- CHILD GETTING ON/OFF SCHOOL BUS |
56- RIDING ACROSS ROAD |
7- WESTBOUND |
|
|
N |
|
|
|
|||||
37- FAIL TO YIELD RIGHT OF WAY TO TRAFFIC |
44- PERSON GETTING ON/OFF VEHICLE |
57- SLOWING/STOPPING/STARTING |
8- NORTH WESTBOUND |
|
|
|
|
|
||||||
38- INATTENTION/DISTRACTION |
|
45- PUSHING/WORKING ON VEHICLE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
8 |
1 |
2 |
|
|
|||||||
39- WALKING/RUNNING IN ROAD WITH TRAFFIC |
46- WORKING IN ROADWAY |
90- OTHER |
|
|
|
|||||||||
|
|
|
|
|
||||||||||
W |
|
7 |
|
|
3 |
|
E |
|||||||
|
|
|
47- PLAYING IN ROADWAY |
|
|
|
|
|
||||||
|
|
|
|
6 |
|
|
4 |
|
||||||
|
|
|
48- NOT IN ROADWAY |
|
|
|
5 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CONTINUE |
|
WAS THERE A POLICE |
|
IF YES, WHAT DEPARTMENT (NAME OF CITY, COUNTY OR STATE PATROL) |
|
|
||||||||
|
|
|
|
|||||||||||
|
OFFICER AT THE |
|
|
|
|
|
|
|
|
|
|
|
||
REPORT ON |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SCENE? |
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER SIDE |
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
MY |
VEHICLE |
OTHER |
| Fact Name | Description |
|---|---|
| Mandatory Submission | Drivers involved in an accident with $1,000 or more in property damage, or any injury or death, are required to complete and submit the Minnesota Accident Report form within 10 days of the incident. |
| Legal Consequences | Failure to submit the report is classified as a misdemeanor under Minnesota Statute 169.09, subdivision 7, which may result in legal repercussions. |
| Data Privacy | The information collected on this form is subject to the Minnesota Data Privacy Act, ensuring that certain data may only be disclosed as specified by law. |
| Form Availability | The Minnesota Accident Report form can be accessed online as an E-form at www.mndriveinfo.org, facilitating easier completion and submission. |
Completing the Minnesota Accident Report form is essential for documenting the details of a vehicle accident. After filling out the form, it must be submitted to Driver and Vehicle Services within 10 days. Ensure that all sections are completed accurately to avoid any issues.
What is the purpose of the Minnesota Accident Report form?
The Minnesota Accident Report form is designed to collect essential information about motor vehicle accidents. This data helps authorities analyze traffic incidents to improve road safety. It is mandatory for drivers involved in accidents with $1,000 or more in property damage, or any injury or death, to complete and submit this form.
Who is required to complete the form?
Every driver involved in a crash that results in significant property damage, injury, or death must complete the Minnesota Accident Report form. This requirement applies regardless of fault. Failure to submit the report can lead to misdemeanor charges under Minnesota law.
How long do I have to submit the report?
Drivers must submit the Minnesota Accident Report form within 10 days of the accident. Timely submission is crucial to avoid penalties and ensure that all necessary information is recorded accurately.
Where do I send the completed form?
The completed Minnesota Accident Report form should be mailed to the following address: DVS / Accident Records, 445 Minnesota Street, Suite 181, St. Paul, MN 55101-5181. Ensure that the form is sent to the correct address to avoid delays in processing.
What information is required on the form?
The form requires detailed information, including the date, time, and location of the accident, as well as details about the vehicles involved, drivers, and any injuries sustained. Insurance information must also be provided. Completing all sections accurately helps facilitate the investigation and record-keeping process.
Is the information on the form confidential?
While the information collected on the Minnesota Accident Report form is used for statistical purposes, certain details may be disclosed under Minnesota law to parties involved in the accident. However, your version of events is treated as confidential and cannot be used against you in legal proceedings.
What happens if I don’t submit the report?
Failing to submit the Minnesota Accident Report form within the required timeframe can result in misdemeanor charges. This can lead to fines and other legal consequences. It is essential to comply with this requirement to avoid potential legal issues.
Failing to provide complete information. Every section of the form must be filled out accurately. Missing details can lead to delays or complications.
Not submitting the report within the required timeframe. The form must be sent to Driver and Vehicle Services within 10 days of the accident.
Inaccurate accident location. Clearly indicate whether the accident occurred at an intersection or on a specific road. This information is crucial for proper documentation.
Omitting insurance details. Provide complete liability insurance information. If this is missing, it will be assumed that you did not have insurance at the time of the accident.
Not including all involved parties. If there are multiple vehicles, ensure that all drivers and passengers are listed correctly. This includes their names, addresses, and other relevant details.
Using unclear or vague descriptions of the accident. Clearly describe what happened and include any relevant details that can help explain the circumstances.
Neglecting to sign the report. The signature of the person submitting the report is required. Without it, the report may not be accepted.
The Minnesota Accident Report form is a critical document for drivers involved in a crash. In addition to this form, there are several other documents that may be required or helpful in the aftermath of an accident. Below is a list of these documents, along with a brief description of each.
These documents can play a vital role in the resolution of any claims or legal matters that arise from an accident. It is essential to gather and retain all relevant information to ensure proper handling of the situation.
The Minnesota Accident Report form shares similarities with the Uniform Accident Report (UAR) used in various states across the U.S. Like the Minnesota form, the UAR is designed to collect essential details about motor vehicle accidents. This includes information about the drivers, vehicles involved, and the circumstances surrounding the incident. Both forms aim to provide a standardized method for reporting accidents, ensuring that law enforcement and insurance companies have access to consistent data for analysis and processing claims.
Another comparable document is the California Traffic Collision Report. This report, much like the Minnesota form, requires drivers involved in accidents to provide detailed information about the event, including the location, time, and nature of the crash. The California report also emphasizes the importance of submitting the information promptly to facilitate investigations and assist in improving road safety, similar to the requirements outlined in the Minnesota form.
The National Highway Traffic Safety Administration (NHTSA) Form 578, which is used for reporting crashes involving commercial vehicles, bears a resemblance to the Minnesota Accident Report. Both forms focus on gathering comprehensive data about the accident, including vehicle types, driver information, and environmental conditions. The NHTSA form specifically addresses the unique aspects of commercial vehicle incidents, while the Minnesota form encompasses a broader range of motor vehicle accidents.
Additionally, the New York State Motor Vehicle Accident Report is similar in purpose and structure. This report collects vital information about the accident, including driver details, vehicle descriptions, and a narrative of the incident. Both reports serve as official documents that can be used by law enforcement and insurance companies to assess liability and damages, reinforcing the importance of accurate reporting in the aftermath of a crash.
The Texas Motor Vehicle Accident Report is another document that aligns closely with the Minnesota form. It requires drivers to detail the circumstances of the accident, including the involved parties and any injuries sustained. Both forms aim to capture critical information that can aid in legal proceedings and insurance claims, emphasizing the necessity of thorough and timely reporting.
The Florida Traffic Crash Report shares similar objectives with the Minnesota Accident Report. Both forms collect data on the accident's specifics, such as the types of vehicles involved and the conditions at the time of the crash. They serve to inform state agencies and contribute to the development of safer roadways, highlighting the shared goal of reducing accidents and improving public safety.
Finally, the Washington State Collision Report is comparable in its focus on gathering detailed information about traffic incidents. Like the Minnesota form, it requires participants to provide information about the vehicles, drivers, and circumstances leading to the crash. This report aims to facilitate law enforcement investigations and insurance claims, underlining the necessity of accurate and timely documentation in the event of an accident.
Things to Do When Filling Out the Minnesota Accident Report Form:
Things Not to Do When Filling Out the Minnesota Accident Report Form:
This is incorrect. The Minnesota Accident Report form must be completed for any crash involving $1,000 or more in property damage, or any injury or death. It is a requirement.
The form must be submitted within 10 days of the accident. Delaying this can lead to legal consequences.
While the driver is primarily responsible, all parties involved should ensure their information is included for accuracy.
The report is confidential and cannot be used as evidence in civil or criminal matters. Your version of events remains protected.
If you lack insurance, you must still submit the form. Failure to do so can result in penalties.
The report is also necessary for accidents involving pedestrians, bicycles, and other non-motorized vehicles.
While an electronic version is available, it must still be printed and mailed to the appropriate address after completion.
Some information is protected under the Minnesota Data Privacy Act, ensuring that personal details are kept confidential.
Filling out the Minnesota Accident Report form is an important step after a vehicle accident. Understanding how to complete this form correctly can make a significant difference in the outcome of your situation. Here are some key takeaways to keep in mind:
Completing the Minnesota Accident Report form thoughtfully and accurately can help protect your rights and ensure that the necessary information is on record. Take your time to fill it out carefully.