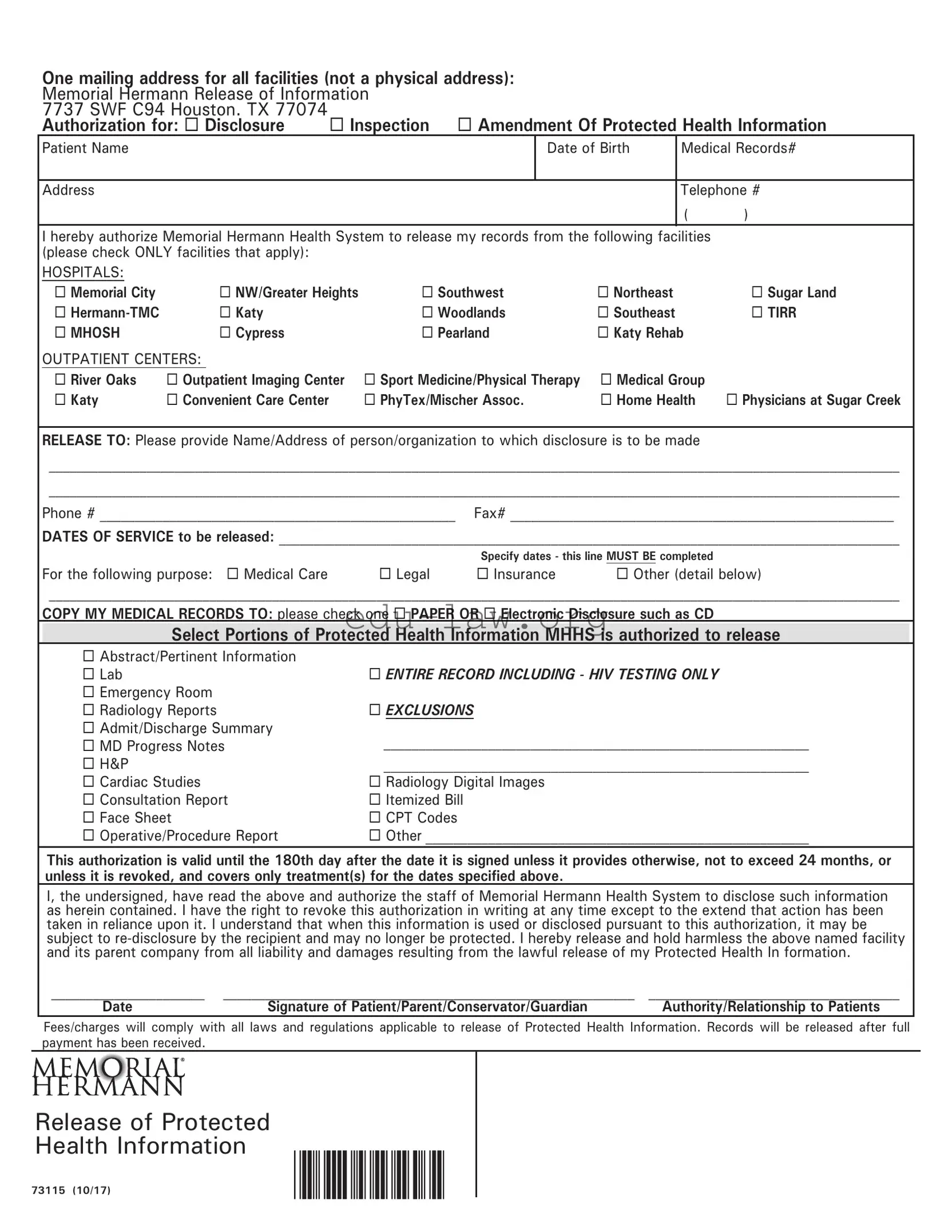
The Memorial Hermann Release form is an essential document that allows patients to authorize the release of their protected health information. It is designed for use across various facilities within the Memorial Hermann Health System, including hospitals and outpatient centers. Patients must provide their personal information, such as name, date of birth, and contact details, along with the specific facilities from which they wish to obtain records. The form requires individuals to specify the dates of service and the purpose for which the records are needed, such as for medical care, legal matters, or insurance purposes. Patients can choose whether they want their medical records in paper or electronic format. Additionally, the form outlines the types of information that can be disclosed, including lab results, emergency room visits, and progress notes. It is crucial to note that the authorization remains valid for 180 days unless revoked or specified otherwise. By signing the form, patients acknowledge their understanding of the potential risks associated with the release of their information and agree to hold the facility harmless from any liability related to the disclosure. This process ensures that patients maintain control over their medical records while facilitating necessary access for various needs.
One mailing address for all facilities (not a physical address): |
|
|
|
||||
Memorial Hermann Release of Information |
|
|
|
||||
7737 SWF C94 Houston. TX 77074 |
Inspection Amendment Of Protected Health Information |
||||||
Authorization for: Disclosure |
|||||||
Patient Name |
|
|
|
Date of Birth |
Medical Records# |
||
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Telephone # |
|
|
|
|
|
|
|
( |
) |
I hereby authorize Memorial Hermann Health System to release my records from the following facilities |
|
||||||
(please check ONLY facilities that apply): |
|
|
|
|
|
|
|
HOSPITALS: |
|
|
|
|
|
|
|
Memorial City |
NW/Greater Heights |
Southwest |
Northeast |
|
Sugar Land |
||
|
Katy |
|
Woodlands |
Southeast |
|
TIRR |
|
MHOSH |
Cypress |
|
Pearland |
Katy Rehab |
|
||
OUTPATIENT CENTERS: |
|
|
|
|
|
|
|
River Oaks |
Outpatient Imaging Center |
Sport Medicine/Physical Therapy |
Medical Group |
|
|||
Katy |
Convenient Care Center |
|
PhyTex/Mischer Assoc. |
Home Health |
Physicians at Sugar Creek |
||
RELEASE TO: Please provide Name/Address of person/organization to which disclosure is to be made
__________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________
Phone # ___________________________________________________ Fax# _______________________________________________________
DATES OF SERVICE to be released: _________________________________________________________________________________________
|
|
Specify dates - this line MUST BE completed |
|
For the following purpose: Medical Care |
Legal |
Insurance |
Other (detail below) |
__________________________________________________________________________________________________________________________
COPY MY MEDICAL RECORDS TO: please check one PAPER OR Electronic Disclosure such as CD
Select Portions of Protected Health Information MHHS is authorized to release
Abstract/Pertinent Information |
|
Lab |
ENTIRE RECORD INCLUDING - HIV TESTING ONLY |
Emergency Room |
|
Radiology Reports |
EXCLUSIONS |
Admit/Discharge Summary |
_____________________________________________________________ |
MD Progress Notes |
|
H&P |
_____________________________________________________________ |
Cardiac Studies |
Radiology Digital Images |
Consultation Report |
Itemized Bill |
Face Sheet |
CPT Codes |
Operative/Procedure Report |
Other _______________________________________________________ |
This authorization is valid until the 180th day after the date it is signed unless it provides otherwise, not to exceed 24 months, or
unless it is revoked, and covers only treatment(s) for the dates specified above.
I, the undersigned, have read the above and authorize the staff of Memorial Hermann Health System to disclose such information as herein contained. I have the right to revoke this authorization in writing at any time except to the extend that action has been taken in reliance upon it. I understand that when this information is used or disclosed pursuant to this authorization, it may be subject to
______________________ |
___________________________________________________________ |
____________________________________ |
Date |
Signature of Patient/Parent/Conservator/Guardian |
Authority/Relationship to Patients |
Fees/charges will comply with all laws and regulations applicable to release of Protected Health Information. Records will be released after full payment has been received.
Release of Protected
Health Information
73115 (10/17)
| Fact Name | Fact Description |
|---|---|
| Mailing Address | The mailing address for all facilities is Memorial Hermann Release of Information, 7737 SWF C94, Houston, TX 77074. |
| Authorization Types | Patients can authorize the release of their medical records for various purposes, including medical care, legal, and insurance. |
| Validity Period | This authorization remains valid until 180 days after the date it is signed, unless revoked or specified otherwise, not exceeding 24 months. |
| Disclosure Options | Patients can choose to receive their medical records in paper or electronic format, such as a CD. |
| Facility Selection | Patients must select the specific Memorial Hermann facilities from which they wish to release records, including various hospitals and outpatient centers. |
| Governing Law | The release of protected health information is governed by Texas state laws regarding medical records and patient privacy. |
After completing the Memorial Hermann Release form, it will be submitted to the designated address. This process allows for the authorized release of medical records. Make sure to provide accurate information to avoid delays in processing.
What is the purpose of the Memorial Hermann Release form?
The Memorial Hermann Release form allows patients to authorize the release of their medical records. This form is essential for facilitating communication between healthcare providers, legal representatives, and insurance companies. It ensures that the patient's protected health information is shared with the appropriate parties for specified purposes, such as medical care, legal matters, or insurance claims.
How do I fill out the Memorial Hermann Release form?
To complete the form, start by providing your personal information, including your name, date of birth, address, and telephone number. Next, select the facilities from which you wish to release records. Specify the recipient's name and address, along with their phone and fax numbers. Indicate the dates of service for which you are requesting records and select the purpose of the release. Finally, choose whether you prefer to receive your records in paper or electronic format, and sign the form.
What facilities can I select on the form?
You can choose from a variety of Memorial Hermann facilities, including hospitals such as Memorial City, Hermann-TMC, and Sugar Land, as well as outpatient centers like River Oaks and Convenient Care Center. Ensure you check only the facilities relevant to your request.
How long is the authorization valid?
The authorization granted by the Memorial Hermann Release form is valid for 180 days from the date of signing. However, it cannot exceed 24 months unless stated otherwise. You have the right to revoke this authorization in writing at any time, except to the extent that action has already been taken based on the authorization.
Can I specify which parts of my medical records to release?
Yes, the form allows you to specify which portions of your protected health information you want to be released. Options include lab results, emergency room records, and even entire records, including HIV testing. You can also exclude certain information if desired.
What should I do if I want to revoke my authorization?
If you wish to revoke your authorization, you must do so in writing. This written revocation should be sent to the appropriate facility or department at Memorial Hermann. Keep in mind that revocation will not affect any actions taken in reliance on the authorization prior to its revocation.
Are there any fees associated with obtaining my medical records?
Yes, there may be fees or charges associated with the release of your protected health information. These fees will comply with applicable laws and regulations. Records will be released only after full payment has been received.
What happens if my records are shared with a third party?
When your information is disclosed pursuant to the authorization, it may be subject to re-disclosure by the recipient. This means that once your records are shared, they may no longer be protected under the same privacy regulations. Therefore, it is important to consider the implications of sharing your health information with third parties.
Who can sign the Memorial Hermann Release form on my behalf?
The form can be signed by the patient, a parent, conservator, or guardian. The individual signing must have the authority to act on behalf of the patient. It is crucial to indicate the relationship to the patient clearly on the form to ensure proper authorization.
Not Providing Complete Patient Information: Failing to fill out the patient's name, date of birth, or medical records number can lead to delays. All sections must be completed accurately to ensure proper identification.
Missing Facility Selection: It's crucial to check only the facilities that apply. Leaving this section blank can result in incomplete records being released or unnecessary delays in processing the request.
Omitting Dates of Service: The section specifying the dates of service must be filled out. If this line is left blank, the request may be considered invalid, causing further complications.
Not Understanding the Purpose of Release: Selecting a purpose without fully understanding it can lead to confusion. Ensure you choose the correct option, whether it’s for medical care, legal reasons, or insurance purposes.
The Memorial Hermann Release form is a crucial document that allows patients to authorize the release of their medical records. However, it is often accompanied by other forms and documents that serve various purposes in the healthcare and legal processes. Understanding these additional documents can help individuals navigate their rights and responsibilities more effectively.
Each of these documents plays a vital role in managing healthcare and protecting patient rights. Being familiar with them can empower individuals to make informed decisions regarding their health information and care. Understanding the implications of each form can also help ensure that patients receive the appropriate care and support they need.
The Memorial Hermann Release form shares similarities with the HIPAA Authorization form. Both documents allow patients to authorize the release of their medical information to specific individuals or organizations. The HIPAA Authorization form is designed to comply with the Health Insurance Portability and Accountability Act, ensuring that patients understand their rights regarding their health information. Like the Memorial Hermann Release form, it requires patient identification details, the purpose of the disclosure, and the specific information to be released. This ensures that the patient's consent is informed and that their privacy is protected.
Another document that resembles the Memorial Hermann Release form is the Medical Records Request form. This form is often used by patients to formally request copies of their medical records from healthcare providers. Similar to the Memorial Hermann form, it typically includes sections for patient identification, the specific records requested, and the intended recipient of the records. Both documents emphasize the importance of clarity in the request to ensure that the right information is provided without delay.
The Authorization for Release of Information form is also comparable to the Memorial Hermann Release form. This document is used in various healthcare settings to allow the release of patient information to third parties. Like the Memorial Hermann form, it requires the patient to specify the information to be shared and the purpose of the release. Both forms aim to protect patient privacy while facilitating the necessary sharing of medical information for treatment or other purposes.
The Consent for Treatment form can be seen as another similar document. While primarily focused on giving permission for medical treatment, it often includes sections that allow for the sharing of relevant medical information with other healthcare providers involved in the patient's care. This is akin to the Memorial Hermann Release form, which also seeks to ensure that necessary information is communicated effectively among healthcare professionals to enhance patient care.
The Patient Information Release form is yet another document that aligns closely with the Memorial Hermann Release form. This form is utilized to grant permission for the release of a patient’s medical records to a designated person or organization. Like the Memorial Hermann form, it requires details about the patient and the specific information being released, ensuring that the patient's wishes are clearly articulated and respected.
Additionally, the Authorization for Use or Disclosure of Health Information form bears similarities to the Memorial Hermann Release form. This document is typically used to obtain consent for sharing health information for purposes such as research or legal proceedings. Both forms require patients to provide specific information about what records can be shared and with whom, reinforcing the importance of informed consent in the handling of personal health information.
Finally, the Release of Liability form also shares a connection with the Memorial Hermann Release form. While its primary purpose is to protect healthcare providers from legal claims related to the release of information, it often includes a section where patients acknowledge their understanding of the risks involved in sharing their health information. This is similar to the Memorial Hermann form, which includes a release clause that protects the facility from liability resulting from the lawful release of protected health information.
When filling out the Memorial Hermann Release form, it's essential to ensure accuracy and completeness. Here are some helpful tips on what to do and what to avoid:
This is incorrect. The Memorial Hermann Release form covers various facilities, including outpatient centers and rehabilitation services. It allows you to specify which locations you want your records released from.
This is not true. You must specify the dates of service for the records you want released. Leaving this section blank may result in a denial of your request.
The authorization is valid for a limited time. It lasts until the 180th day after signing, unless you revoke it sooner. It cannot exceed 24 months.
You have the right to revoke your authorization in writing at any time. However, this does not affect actions taken before your revocation.
Fees may apply for the release of your Protected Health Information. The facility will comply with all applicable laws and regulations regarding these charges.
When filling out the Memorial Hermann Release form, keep these key takeaways in mind: