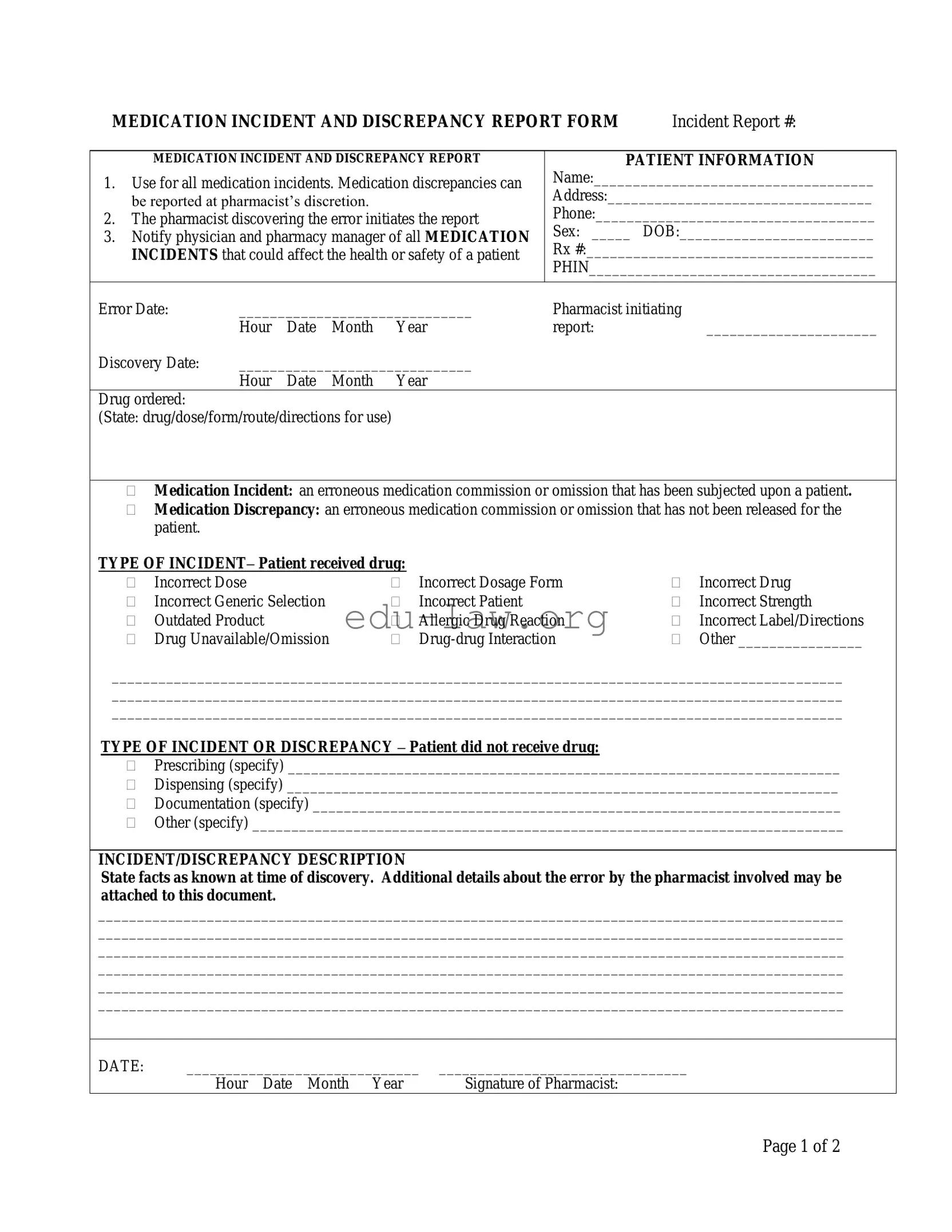
The Medication Error form is an essential tool for documenting incidents related to medication discrepancies in a healthcare setting. It serves to ensure patient safety by capturing critical information about any errors that may have occurred during the prescribing, dispensing, or administration of medications. When a pharmacist identifies a medication error, they are responsible for initiating the report, which includes details such as the patient's information, the nature of the error, and the actions taken in response. This form allows for the classification of incidents, distinguishing between those that have affected the patient and those that have not yet been administered. Additionally, it prompts the pharmacist to notify both the physician and pharmacy manager, emphasizing the importance of communication in addressing potential health risks. The form also includes sections for contributing factors and follow-up actions, enabling a thorough investigation into the root causes of the error. By systematically documenting these incidents, healthcare providers can improve practices and prevent future occurrences, ultimately enhancing patient care.
MEDICATION INCIDENT AND DISCREPANCY REPORT FORM |
Incident Report #: |
MEDICATION INCIDENT AND DISCREPANCY REPORT
1.Use for all medication incidents. Medication discrepancies can be reported at pharmacist’s discretion.
2.The pharmacist discovering the error initiates the report
3.Notify physician and pharmacy manager of all MEDICATION INCIDENTS that could affect the health or safety of a patient
PATIENT INFORMATION
Name:____________________________________
Address:__________________________________
Phone:____________________________________
Sex: _____ DOB:_________________________
Rx #:_____________________________________
PHIN_____________________________________
Error Date: |
______________________________ |
Pharmacist initiating |
|
|||
|
Hour |
Date |
Month |
Year |
report: |
______________________ |
Discovery Date: |
______________________________ |
|
|
|||
|
Hour |
Date |
Month |
Year |
|
|
Drug ordered: |
|
|
|
|
|
|
(State: drug/dose/form/route/directions for use) |
|
|
|
|||
Medication Incident: an erroneous medication commission or omission that has been subjected upon a patient.
Medication Discrepancy: an erroneous medication commission or omission that has not been released for the patient.
TYPE OF INCIDENT– Patient received drug: |
|
|
|
||
|
Incorrect Dose |
|
Incorrect Dosage Form |
|
Incorrect Drug |
|
Incorrect Generic Selection |
|
Incorrect Patient |
|
Incorrect Strength |
|
Outdated Product |
|
Allergic Drug Reaction |
|
Incorrect Label/Directions |
|
Drug Unavailable/Omission |
|
|
Other ________________ |
|
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
TYPE OF INCIDENT OR DISCREPANCY – Patient did not receive drug:
Prescribing (specify) _______________________________________________________________________
Dispensing (specify) _______________________________________________________________________
Documentation (specify) ____________________________________________________________________
Other (specify) ____________________________________________________________________________
INCIDENT/DISCREPANCY DESCRIPTION
State facts as known at time of discovery. Additional details about the error by the pharmacist involved may be attached to this document.
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
DATE: |
______________________________ |
________________________________ |
|
Hour Date Month Year |
Signature of Pharmacist: |
Page 1 of 2
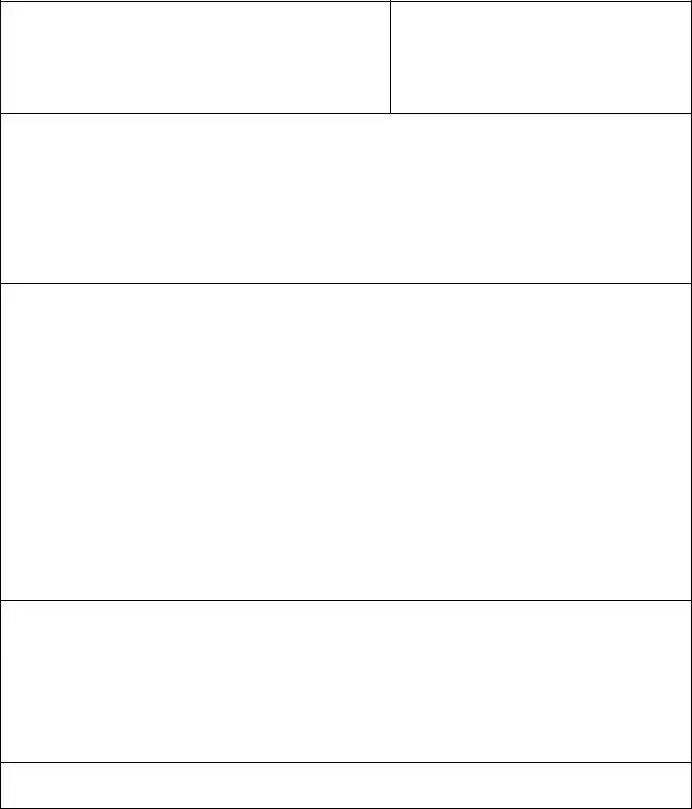
CONTRIBUTING FACTORS
(To be completed by pharmacist responsible)
|
Improper patient identification |
Misread/misinterpreted drug order (include verbal orders) |
|
|
Incorrect transcription |
|
Drug unavailable |
Lack of patient counselling |
|
Other |
|
|
DATE: |
______________________________ |
__________________ |
|
|
||||
|
|
Hour Date Month Year |
Signature |
|
|
|
|||
|
NOTIFICATION – Complete the following information according to Standards of Practice. |
||||||||
1. |
Patient notified: |
|
|
|
|
|
|
|
|
|
|
|
___________________________ |
|
|||||
|
|
|
Hour |
Date |
Month |
Year |
|||
2. |
Physician notified: ____ |
______________________________ |
|
||||||
|
|
Yes/No |
Hour |
Date |
Month |
Year |
|||
|
|
|
|
|
|
|
|
|
|
|
SEVERITY |
|
|
|
|
|
|
|
|
|
|
None |
|
No change in patient’s condition: no medical intervention |
|||||
|
|
Minor |
|
|
|
required |
|
|
|
|
|
Major |
|
Produces a temporary systemic or localized response: does |
|||||
|
|
|
|
|
|
not cause ongoing complications |
|||
|
|
|
|
Requires immediate medical intervention |
|||||
|
OUTCOME OF INVESTIGATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Problem Identification |
|
|
|
Action |
|
|
|
|
|
|
Lack of knowledge |
|
|
Education provided |
||||
|
|
Performance problem |
|
|
Policy/procedure changed |
||||
|
|
Administration problem |
|
|
System changed |
|
|
||
|
|
Other |
|
|
Individual awareness |
||||
|
|
|
|
|
Group awareness |
||||
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|||||
|
RESOLUTION OF PROBLEM THAT RESULTED IN THE ERROR BEING MADE: |
||||||||
|
|
|
|
|
|
|
|
||
|
Signature: |
Date: |
Signature: |
Date: |
|||||
|
(Pharmacist filling out the form) |
|
|
|
(Pharmacy Manager) |
||||
PHARMACY USE ONLY
Page 2 of 2
| Fact Name | Description |
|---|---|
| Purpose of Form | This form is used to report all medication incidents and discrepancies, allowing for improved patient safety. |
| Initiation of Report | The pharmacist who discovers the medication error is responsible for initiating the report. |
| Notification Requirements | All medication incidents that could impact patient health or safety must be reported to the physician and pharmacy manager. |
| Patient Information | The form requires detailed patient information, including name, address, phone number, sex, date of birth, and prescription number. |
| Types of Incidents | Incidents can include incorrect dosage, incorrect drug, allergic reactions, and other discrepancies affecting patient care. |
| Severity Levels | The form categorizes severity from "none" to "requires immediate medical intervention," guiding the response needed. |
| Contributing Factors | Pharmacists must identify contributing factors such as improper patient identification or misread drug orders. |
| Follow-Up Actions | Investigations may lead to actions such as education provided, policy changes, or system adjustments to prevent future errors. |
| State-Specific Regulations | Each state may have specific laws governing the reporting of medication errors, ensuring compliance with local regulations. |
Completing the Medication Error form is an important step in ensuring patient safety and improving pharmacy practices. Once you have filled out the form, it should be submitted to the appropriate authorities for review and follow-up actions. This process helps in identifying areas for improvement and preventing future incidents.
What is the purpose of the Medication Error form?
The Medication Error form is designed to document any medication incidents or discrepancies that occur during the medication process. This includes errors made in prescribing, dispensing, or administering medications. The goal is to ensure patient safety by identifying and addressing issues that could potentially harm patients. By reporting these incidents, healthcare professionals can learn from mistakes and implement changes to prevent future occurrences.
Who is responsible for initiating the report?
The pharmacist who discovers the medication error is responsible for initiating the report. This is crucial as it allows for immediate documentation of the incident, ensuring that all relevant details are captured accurately. Once the report is completed, it should be communicated to the physician and the pharmacy manager, especially if the incident could impact the health or safety of a patient.
What types of incidents should be reported using this form?
There are various types of incidents that can be reported using the Medication Error form. These include, but are not limited to, incorrect dosing, incorrect medication forms, and allergic reactions. If a patient did not receive their medication due to prescribing or dispensing errors, those should also be documented. Each type of incident helps in understanding the nature of errors and the necessary steps to mitigate them.
How should the incident or discrepancy be described in the report?
In the report, the pharmacist should provide a clear and factual description of the incident as known at the time of discovery. This includes detailing what happened, when it happened, and any other relevant information that could help in the investigation. Additional details may be attached to the form if necessary. The more comprehensive the description, the better the understanding of the incident and its contributing factors.
What happens after the report is submitted?
After the Medication Error form is submitted, it undergoes an investigation to identify the root cause of the error. The pharmacist responsible will complete a section detailing contributing factors and possible resolutions. Follow-up actions may include providing education, changing policies, or improving systems to prevent similar errors in the future. The outcomes of these investigations are vital for enhancing patient safety and improving pharmacy practices.
Incomplete Patient Information: Failing to fill out all required fields, such as the patient's name, address, or date of birth, can lead to confusion and hinder proper follow-up.
Not Specifying the Type of Incident: Selecting multiple incident types without clear specification can make it difficult to assess the situation accurately. Always choose the most relevant category and provide details.
Insufficient Description of the Incident: Providing vague or unclear descriptions in the incident section can result in misunderstandings. Be as detailed as possible about what occurred.
Neglecting to Notify Key Individuals: Not notifying the physician or pharmacy manager can delay necessary actions. Ensure all relevant parties are informed promptly.
Missing Signatures: Forgetting to sign the report can render it invalid. Both the initiating pharmacist and the pharmacy manager must sign the form to confirm its accuracy.
When addressing medication errors, several additional forms and documents can aid in providing a comprehensive overview of the incident. These documents serve various purposes, from tracking the error to ensuring proper communication among healthcare professionals. Below is a list of commonly used forms that complement the Medication Error form.
Utilizing these documents alongside the Medication Error form enhances the overall approach to medication safety. Each form plays a critical role in fostering a culture of accountability, transparency, and continuous improvement within healthcare settings.
The Incident Report is a foundational document used across various healthcare settings to capture details about any event that deviates from the standard of care. Similar to the Medication Error form, it aims to document incidents affecting patient safety. The report includes essential information such as the date, time, and nature of the incident, which allows healthcare professionals to analyze trends and implement preventive measures. Both documents emphasize the importance of transparency and communication among healthcare providers, ensuring that all parties involved are informed and can take appropriate action.
The Adverse Event Report serves a similar purpose by documenting any unintended harm that occurs as a result of medical care. Like the Medication Error form, it focuses on capturing specific details about the incident, including the patient's condition and the treatment provided. This report is critical for understanding the impact of medical interventions and improving patient safety. Both documents require timely completion and notification of relevant parties, fostering a culture of accountability and continuous improvement within healthcare organizations.
The Quality Assurance Report is another document that aligns with the Medication Error form in its goal of enhancing patient safety. This report evaluates the effectiveness of healthcare practices and identifies areas for improvement. It often includes data on medication errors, allowing organizations to analyze patterns and implement corrective actions. Both documents contribute to a systematic approach to quality improvement, ensuring that patient care is continuously monitored and refined based on real-world experiences.
The Root Cause Analysis Report delves deeper into incidents, including medication errors, to identify underlying causes. This document is similar to the Medication Error form in that it seeks to prevent future occurrences by analyzing contributing factors. By focusing on systemic issues rather than individual mistakes, both documents promote a proactive approach to safety. The findings from a Root Cause Analysis can lead to significant changes in policies and procedures, thereby enhancing overall patient care.
The Pharmacy Audit Report also shares similarities with the Medication Error form, particularly in its role in monitoring compliance with medication management standards. This report assesses the accuracy of medication dispensing and administration processes, highlighting discrepancies that may lead to errors. Both documents aim to ensure that pharmacists adhere to best practices, thereby safeguarding patient health. Regular audits, like those documented in the Pharmacy Audit Report, can identify trends in medication errors, prompting necessary training or policy adjustments.
The Medication Reconciliation Form is another document that parallels the Medication Error form in its focus on ensuring patient safety during transitions of care. It documents the patient’s medication history and any changes made during treatment. Both forms emphasize the importance of accurate medication management and communication among healthcare providers. Effective medication reconciliation can prevent errors related to omissions or duplications, reinforcing the goal of providing safe and effective patient care.
Finally, the Incident Command System (ICS) Report, often used in emergency situations, bears similarities to the Medication Error form in its structured approach to documenting incidents. The ICS Report captures critical information about the response to an emergency, including any medication-related errors that may occur during high-pressure situations. Both documents prioritize clear communication and systematic documentation, ensuring that all relevant details are recorded for future analysis and improvement in patient safety protocols.
When filling out the Medication Error form, it’s important to ensure accuracy and clarity. Here are some essential dos and don’ts to keep in mind:
Misconceptions about the Medication Error form can lead to confusion and hinder the reporting process. Here are six common misunderstandings:
Understanding these misconceptions can foster a culture of safety and encourage open communication about medication errors. By addressing these misunderstandings, everyone involved can contribute to better patient care.
When it comes to filling out and using the Medication Error form, understanding its purpose and process is essential for ensuring patient safety. Here are some key takeaways to keep in mind:
By keeping these takeaways in mind, you can help create a safer environment for patients and ensure that medication errors are addressed effectively.