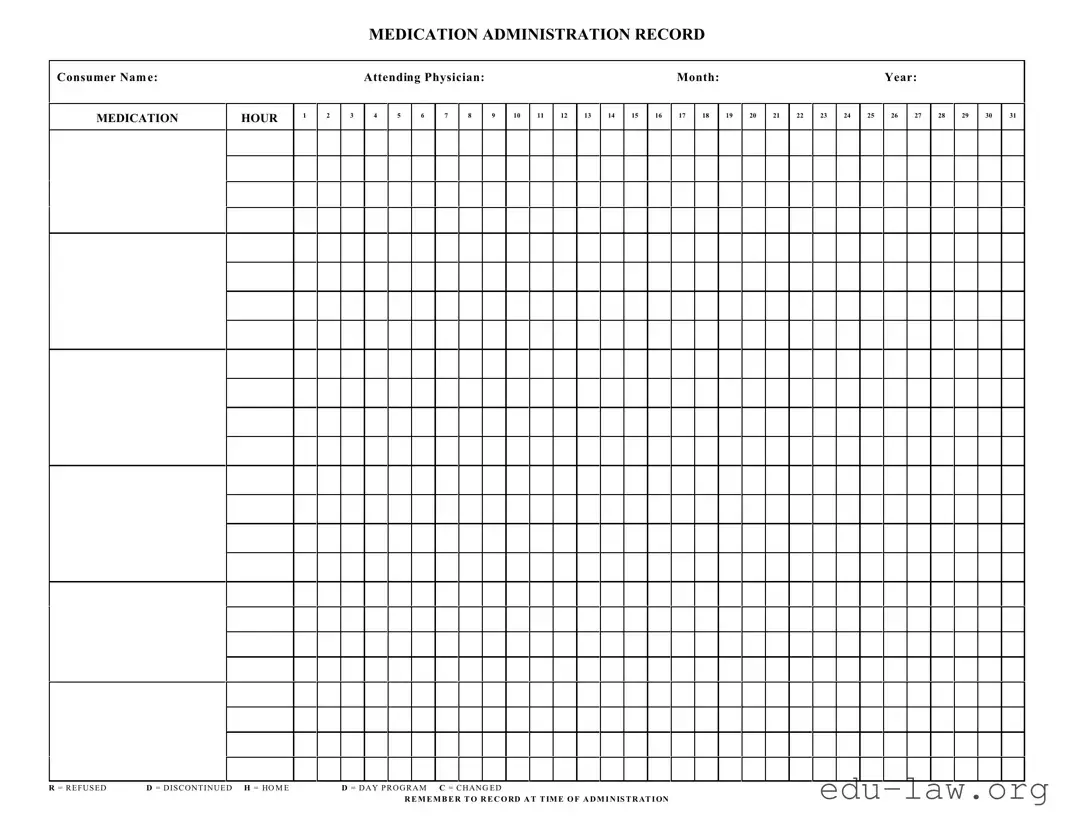
The Medication Administration Record Sheet, often abbreviated as MAR, plays a critical role in ensuring effective medication management for patients. Designed to track the administration of medications, it includes essential details such as the consumer's name, attending physician, and the specific month and year. Each hour of the day is carefully outlined, allowing healthcare professionals to document when each medication is administered. The form also accommodates various notations: 'R' indicates medication was refused, 'D' signifies discontinuation, 'H' pertains to medications administered at home, and 'D' for those given during day programs, while 'C' indicates a change in the medication regimen. This structured format not only supports accurate record-keeping but also serves as a vital communication tool among the care team. Remember, timely and accurate recording on the MAR is essential to ensure patients receive their medications as intended, minimizing the risk of omissions or errors.
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
| Fact Name | Fact Description |
|---|---|
| Purpose | The Medication Administration Record Sheet is designed to track when medications are given to patients. |
| Consumer Information | The form must include the consumer's name and details to ensure accountability and proper record-keeping. |
| Time Reporting | Hours are recorded in a clear format, allowing staff to easily see when each medication has been administered. |
| State Compliance | In some states, the use of this form is governed by laws such as the Nurse Practice Act or specific health regulations. |
| Documentation Notes | Staff must remember to record any refusals, discontinuations, or changes in administration at the time of giving medication. |
Filling out a Medication Administration Record Sheet is an essential task that helps ensure accurate tracking of medication administration. Following a systematic process can make the completion of this form more straightforward.
What is a Medication Administration Record Sheet?
The Medication Administration Record Sheet, often referred to as MAR, is a form used to document the medications given to patients. It helps track what medications are administered, the dosages, and the times they were taken. This record is essential for ensuring that patients receive their medications correctly and consistently.
Who should fill out the Medication Administration Record Sheet?
Healthcare providers who administer medications are responsible for filling out the Medication Administration Record Sheet. This may include nurses, nursing assistants, or other qualified personnel. Accurate completion of this form helps maintain medication safety and compliance.
What information is required on the form?
The Medication Administration Record Sheet requires several key pieces of information. This includes the patient's name, attending physician's name, the month and year, the time of administration, and the specific medications administered for each hour. Each medication should be noted along with any relevant codes, such as R for refused or D for discontinued.
How do I interpret the codes on the form?
Coded entries on the Medication Administration Record Sheet provide quick reference for tracking medication status. For instance, R stands for "refused," indicating the patient did not take the medication, while D signifies "discontinued," meaning the medication is no longer prescribed. Using these codes maintains clarity and improves communication among healthcare providers.
Why is it important to record medication administration at the time of giving?
Recording medication administration at the time it occurs is crucial for several reasons. It helps ensure accuracy, prevents errors, and provides an up-to-date account of the patient's medication history. This practice is essential for both patient safety and effective communication among the healthcare team.
What should I do if I forget to record a medication?
If a medication administration is forgotten, it is important to document it as soon as you realize the oversight. Write down the time and reason for the missed record, and notify the attending healthcare provider. This helps maintain an accurate medical history and allows for appropriate follow-up actions.
Can the Medication Administration Record Sheet be used for different types of medications?
Yes, the Medication Administration Record Sheet can document various types of medications, including oral, injectable, and topical forms. Regardless of the method of administration, ensuring accurate records helps facilitate proper patient care and medication management.
What happens if a medication dosage changes?
If there is a change in a medication dosage, it should be clearly noted on the Medication Administration Record Sheet. Record the new dosage in the appropriate time slot and indicate any changes in prescribing instructions. This ensures that all healthcare providers are aware of the updated medication regimen.
How do I handle a situation where a patient refuses medication?
If a patient refuses medication, you must document the refusal accurately on the Medication Administration Record Sheet using the code "R." Additionally, try to understand the reason for the refusal and inform the attending healthcare provider. This approach allows for a prompt investigation and can help address any patient concerns.
Is the Medication Administration Record Sheet legally binding?
Yes, the Medication Administration Record Sheet serves as a legal document in healthcare settings. It provides a formal record of medication administration, and inaccuracies or omissions may have legal implications. Therefore, it is crucial to complete the form diligently and accurately to protect both patient rights and the healthcare providers involved.
Incomplete Consumer Information: Always ensure that the consumer's name is fully and correctly entered at the top of the sheet. Missing or misspelled names can create confusion and lead to administration errors.
Ignoring the Date and Time: It is crucial to accurately fill in the month and year, along with the corresponding administration hour. Failing to do so might result in the wrong medication being given at the wrong time.
Failure to Record Administration: Remember to mark each time medication is administered. Whether it is done correctly or refused, there should be a record. Not recording can have significant implications for both the patient’s health and legal obligations.
Misunderstanding Codes: Familiarize yourself with the abbreviations such as R for Refused, D for Discontinued, and H for Home. Misinterpretation may lead to incorrect entries that can compromise patient care.
Neglecting to Update Changes: If there are changes in medication or instructions from the attending physician, these must be documented promptly. Failing to update can lead to administering outdated or incorrect dosages.
The Medication Administration Record Sheet is an essential document used for tracking the administration of medications to consumers. It is often accompanied by various other forms and documents that ensure comprehensive management of medication practices and patient care. Below is a list of commonly used forms that complement the Medication Administration Record Sheet.
Each of these documents plays a significant role in ensuring safe and effective medication management. Proper utilization of these forms contributes to a higher standard of patient care and enhances communication among healthcare providers.
The Medication Administration Record (MAR) is similar to a Patient Chart, which serves as a comprehensive documentation of a patient’s medical history. This chart includes vital information such as previous diagnoses, treatments, and tests. Like the MAR, the Patient Chart is utilized as a reference tool for healthcare professionals to ensure that care is consistent and informed. Both documents require accurate recording and serve the purpose of tracking a patient's progress over time.
Another document closely related to the MAR is the Progress Note. Progress Notes are frequently used by healthcare providers to update the patient's status during treatment. These notes include observations, treatment responses, and any changes made in the treatment plan. While the MAR specifically focuses on medication administration, Progress Notes provide a broader context of the overall care a patient is receiving, thus serving as complementary records in patient management.
The Medication List is also quite similar to the MAR. This document outlines all medications a patient is currently taking, including dosages and administration times. Like the MAR, the Medication List is crucial for preventing medication errors and ensuring safe pharmaceutical practices. Its streamlined format makes it easy for health providers to quickly reference the medications being prescribed or administered in various care settings.
Another related document is the Treatment Plan. A Treatment Plan outlines specific health goals and the interventions proposed to achieve them. It often includes medication management as part of the overall strategy. Both the Treatment Plan and the MAR are essential in ensuring coordination among healthcare providers and in offering a structured approach to patient care by documenting intended treatments and actual administrations.
Additionally, the Incident Report bears similarities to the MAR. This report is used when there is an unexpected event during medication administration, such as an allergic reaction or error. While the MAR tracks medication given, Incident Reports focus on documenting deviations from standard procedures. Both documents contribute to improving patient safety and quality of care by allowing healthcare institutions to assess and address issues as they arise.
Lastly, the Nursing Care Plan is reminiscent of the MAR in that it outlines nursing interventions necessary for patient care, which can include medication management. The Nursing Care Plan is broader in its scope, often detailing various aspects of care beyond medication. Yet, like the MAR, it ensures that all healthcare team members are aware of the specific actions required to effectively care for the patient, reinforcing consistency and coordination in treatment methods.
Things to Do:
Things to Avoid:
Understanding the Medication Administration Record Sheet (MARS) is crucial for proper medication management. Unfortunately, misconceptions about this form can lead to errors in medication administration and documentation. Here are ten common misconceptions:
Addressing these misconceptions can enhance patient safety and ensure medication management is both effective and compliant with best practices.
When utilizing the Medication Administration Record Sheet form, it is essential to be mindful of several key points that ensure accurate documentation and effectiveness in administering medications.
Free Gift Card Template - This certificate transforms every shopping trip into a special occasion.
High School Transcript - A critical component of any academic portfolio presented to colleges.