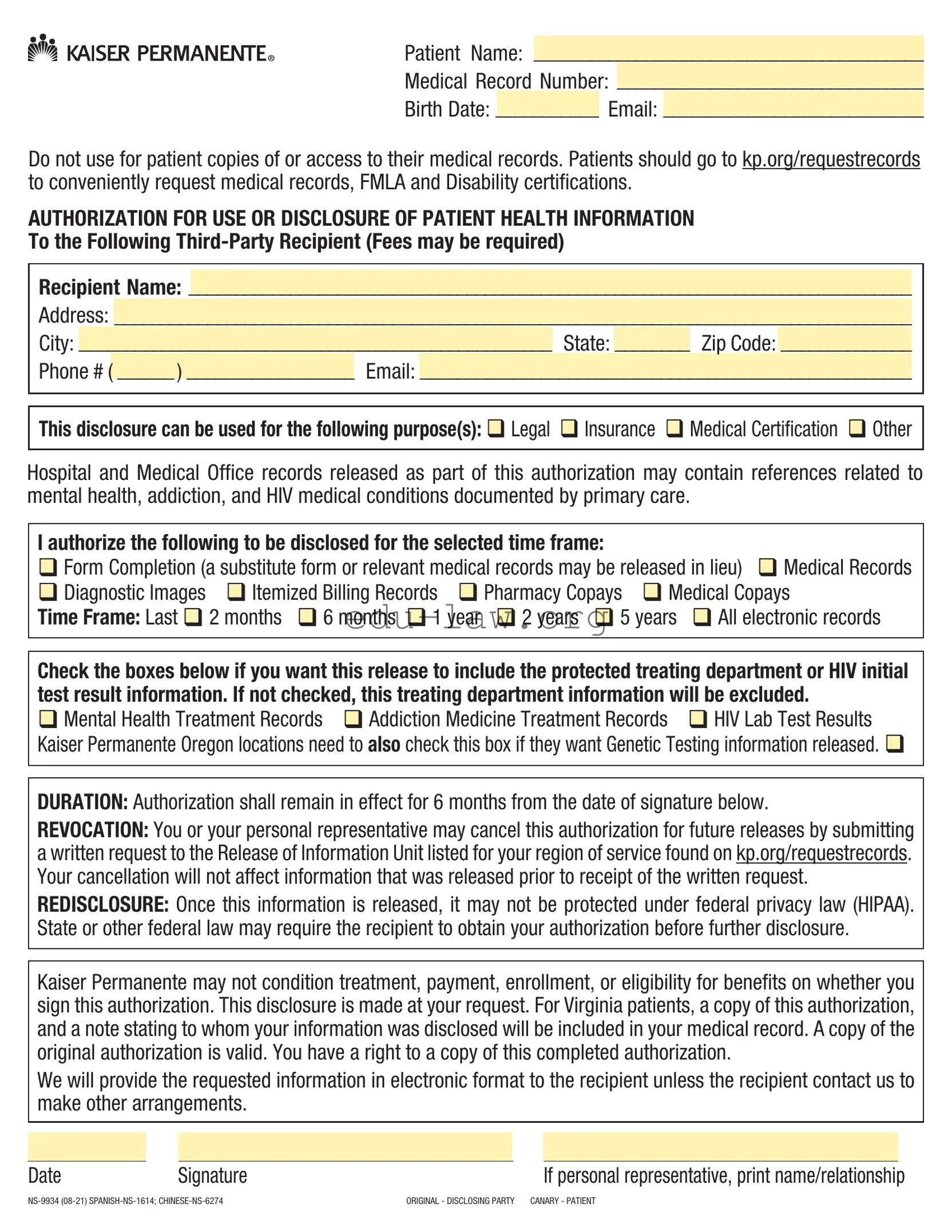
The Kaiser Records Request form is an essential tool for individuals seeking to authorize the release of their medical information to a third party. This form captures crucial details such as the patient's name, medical record number, and contact information. It is important to note that this form is not intended for patients to access their own medical records; instead, they should visit kp.org/requestrecords for that purpose. The form allows patients to specify the recipient of the information, which can include legal, insurance, or medical certification purposes. It also offers options for the type of information to be disclosed, including medical records, diagnostic images, and billing records. Patients can choose a time frame for the records, ranging from the last two months to five years, or even all electronic records. Special protections are available for sensitive information related to mental health, addiction, and HIV. The authorization remains valid for six months, and patients have the right to revoke it at any time. Understanding how to properly fill out this form is crucial for ensuring that the necessary information is shared securely and efficiently.
Patient Name: __________________________________________
Medical Record Number: _________________________________
Birth Date: ___________ Email: ____________________________
Do not use for patient copies of or access to their medical records. Patients should go to kp.org/requestrecords to conveniently request medical records, FMLA and Disability certifications.
AUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT HEALTH INFORMATION
To the Following
Recipient Name: ______________________________________________________________________________
Address: ______________________________________________________________________________________
City: ___________________________________________________ State: ________ Zip Code: ______________
Phone # ( ______ ) __________________ Email: _____________________________________________________
This disclosure can be used for the following purpose(s): Legal Insurance Medical Certification Other
Hospital and Medical Office records released as part of this authorization may contain references related to mental health, addiction, and HIV medical conditions documented by primary care.
I authorize the following to be disclosed for the selected time frame:
Form Completion (a substitute form or relevant medical records may be released in lieu) Medical Records
|
Diagnostic Images |
|
|
Itemized Billing Records |
|
Pharmacy Copays |
|
Medical Copays |
||||||||||
|
|
|
||||||||||||||||
|
|
|
|
|||||||||||||||
Time Frame: Last |
|
2 months |
|
6 months |
|
1 year |
2 years |
|
5 years |
|
All electronic records |
|||||||
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|||||||||||||
Check the boxes below if you want this release to include the protected treating department or HIV initial test result information. If not checked, this treating department information will be excluded.
Mental Health Treatment Records Addiction Medicine Treatment Records HIV Lab Test Results Kaiser Permanente Oregon locations need to also check this box if they want Genetic Testing information released.
DURATION: Authorization shall remain in effect for 6 months from the date of signature below.
REVOCATION: You or your personal representative may cancel this authorization for future releases by submitting a written request to the Release of Information Unit listed for your region of service found on kp.org/requestrecords. Your cancellation will not affect information that was released prior to receipt of the written request.
REDISCLOSURE: Once this information is released, it may not be protected under federal privacy law (HIPAA). State or other federal law may require the recipient to obtain your authorization before further disclosure.
Kaiser Permanente may not condition treatment, payment, enrollment, or eligibility for benefits on whether you sign this authorization. This disclosure is made at your request. For Virginia patients, a copy of this authorization, and a note stating to whom your information was disclosed will be included in your medical record. A copy of the original authorization is valid. You have a right to a copy of this completed authorization.
We will provide the requested information in electronic format to the recipient unless the recipient contact us to make other arrangements.
|
|
|
|
|
|
|
Date |
|
Signature |
|
|
If personal representative, print name/relationship |
|
ORIGINAL - DISCLOSING PARTY CANARY - PATIENT |
||||||
Instructions:
1)Complete the patient identification information on the top
2)Complete all required information for the recipient including a valid email address
3)Check the box for purpose of disclosure
4)Check the box(es) for the type of information to be disclosed and also check the box for a timeframe
5)If you want specially protected information to be included, check the appropriate box(es)
6)Enter the date you are signing the authorization
7)Sign the form
8)If you are a personal representative, print your name and relationship. We may reach out for you to provide additional documentation if needed.
9)Submit this form to the third party you are authorizing to obtain records
10)Keep a copy for your records
“Kaiser Permanente” means both your insurance company (a Kaiser Permanente health plan) and your doctors (a Permanente medical or dental group). It also includes different groups depending on where you live.
To find contact information go to kp.org and search locations for your region/market listed below or alternatively go to kp.org/requestrecords and indicate your region/market.
All states where we do business:
•Kaiser Foundation Hospitals
•Kaiser Permanente Insurance Company
Colorado:
•Kaiser Foundation Health Plan of Colorado
•Colorado Permanente Medical Group, P.C.
Georgia:
•Kaiser Foundation Health Plan of Georgia, Inc.
•The Southeast Permanente Medical Group, Inc.
•Kaiser Foundation Health Plan of the
•
Washington:
•Kaiser Foundation Health Plan of Washington
•Washington Permanente Medical Group, P.C.
Hawaii:
•Kaiser Foundation Health Plan, Inc., Hawaii Region
•Hawaii Permanente Medical Group, Inc.
•Maui Health Systems
Northwest (Oregon/SW Washington):
•Kaiser Foundation Health Plan of the Northwest
•Northwest Permanente, P.C.
•Permanente Dental Associates, P.C.
California - North:
•Kaiser Foundation Health Plan, Inc., Northern California Region
•The Permanente Medical Group, Inc.
California - South:
•Kaiser Foundation Health Plan, Inc., Southern California Region
•Southern California Permanente Medical Group
Patient Name: __________________________________________
Medical Record Number: _________________________________
Birth Date: ___________ Email: ____________________________
Do not use for patient copies of or access to their medical records. Patients should go to kp.org/requestrecords to conveniently request medical records, FMLA and Disability certifications.
AUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT HEALTH INFORMATION
To the Following
Recipient Name: ______________________________________________________________________________
Address: ______________________________________________________________________________________
City: ___________________________________________________ State: ________ Zip Code: ______________
Phone # ( ______ ) __________________ Email: _____________________________________________________
This disclosure can be used for the following purpose(s): Legal Insurance Medical Certification Other
Hospital and Medical Office records released as part of this authorization may contain references related to mental health, addiction, and HIV medical conditions documented by primary care.
I authorize the following to be disclosed for the selected time frame:
Form Completion (a substitute form or relevant medical records may be released in lieu) Medical Records
Diagnostic Images |
Itemized Billing Records Pharmacy Copays Medical Copays |
Time Frame: Last |
2 months 6 months 1 year 2 years 5 years All electronic records |
Check the boxes below if you want this release to include the protected treating department or HIV initial test result information. If not checked, this treating department information will be excluded.
Mental Health Treatment Records Addiction Medicine Treatment Records HIV Lab Test Results Kaiser Permanente Oregon locations need to also check this box if they want Genetic Testing information released.
DURATION: Authorization shall remain in effect for 6 months from the date of signature below.
REVOCATION: You or your personal representative may cancel this authorization for future releases by submitting a written request to the Release of Information Unit listed for your region of service found on kp.org/requestrecords. Your cancellation will not affect information that was released prior to receipt of the written request.
REDISCLOSURE: Once this information is released, it may not be protected under federal privacy law (HIPAA). State or other federal law may require the recipient to obtain your authorization before further disclosure.
Kaiser Permanente may not condition treatment, payment, enrollment, or eligibility for benefits on whether you sign this authorization. This disclosure is made at your request. For Virginia patients, a copy of this authorization, and a note stating to whom your information was disclosed will be included in your medical record. A copy of the original authorization is valid. You have a right to a copy of this completed authorization.
We will provide the requested information in electronic format to the recipient unless the recipient contact us to make other arrangements.
|
|
|
|
|
|
|
Date |
Signature |
|
|
If personal representative, print name/relationship |
||
ORIGINAL - DISCLOSING PARTY CANARY - PATIENT |
||||||
| Fact Name | Details |
|---|---|
| Patient Information Required | The form requires essential patient details such as name, medical record number, birth date, and email address. |
| Third-Party Disclosure | Patients can authorize the release of their health information to a specified third-party recipient, which may include legal or insurance purposes. |
| Duration of Authorization | The authorization remains effective for six months from the date of signature, allowing for a limited timeframe for information release. |
| Revocation of Authorization | Patients can revoke their authorization at any time by submitting a written request to the designated Release of Information Unit. |
| Special Protections | Patients can choose to include sensitive information, such as mental health records or HIV lab test results, in their disclosure. |
| State-Specific Regulations | In Virginia, a copy of the authorization and a note of disclosure will be included in the patient's medical record, adhering to state privacy laws. |
Once you have the Kaiser Records Request form in hand, you’ll want to make sure you fill it out accurately. Completing this form is essential for ensuring that your medical records are sent to the right person or organization. Follow these steps carefully to avoid any delays in processing your request.
What is the Kaiser Records Request form used for?
The Kaiser Records Request form is used to authorize the release of your health information to a third party. This can include medical records, diagnostic images, billing records, and more. It is important to note that this form is not for patients requesting their own medical records directly. For that purpose, patients should visit kp.org/requestrecords.
Who can I authorize to receive my medical records?
You can authorize any third party, such as a lawyer, insurance company, or another healthcare provider, to receive your medical records. Be sure to provide their name, address, phone number, and email on the form. This information is essential for ensuring that your records are sent to the correct recipient.
How long is the authorization valid?
The authorization you provide on the Kaiser Records Request form remains in effect for six months from the date you sign it. If you need to revoke the authorization before that period ends, you can do so by submitting a written request to the Release of Information Unit for your region.
What types of information can I request to be disclosed?
You can request various types of information, including medical records, diagnostic images, itemized billing records, and pharmacy copays. Additionally, if you want to include sensitive information such as mental health treatment records, addiction medicine treatment records, or HIV lab test results, you must check the appropriate boxes on the form.
Can I cancel my authorization after I submit the form?
Yes, you can cancel your authorization for future releases at any time. To do this, you need to submit a written request to the Release of Information Unit. However, it is important to note that any information already released prior to your cancellation request will not be affected.
What should I do if I need my medical records urgently?
If you need your medical records quickly, it is advisable to use the online service at kp.org/requestrecords. This platform allows patients to conveniently request their own medical records, FMLA, and disability certifications. This method can be faster than submitting a physical form.
Is there a fee associated with the release of my medical records?
Fees may be required for the release of medical records to a third party. It is essential to check with the recipient of the records regarding any potential costs. Kaiser Permanente does not charge patients for accessing their own medical records through the online portal.
Incomplete Patient Information: Failing to fill out all required fields, such as the patient name, medical record number, and birth date, can delay the processing of the request.
Missing Recipient Details: Not providing complete information for the third-party recipient, including a valid email address, can lead to issues in delivering the requested records.
Omitting Purpose of Disclosure: Forgetting to check the box indicating the purpose of the disclosure may result in confusion about why the records are being requested.
Neglecting Special Information: If you want to include sensitive information, such as mental health or HIV records, failing to check the appropriate boxes will exclude that information from the release.
Not Signing the Form: Forgetting to sign the authorization can render the request invalid, preventing the release of your medical records.
The Kaiser Records Request form is an essential document for patients seeking to authorize the release of their medical records to third parties. However, several other forms and documents may accompany this request to facilitate various processes related to healthcare and patient rights. Below are some commonly used documents in conjunction with the Kaiser Records Request form.
These documents play a crucial role in ensuring that patients can effectively manage their healthcare information and access necessary benefits. Understanding their purpose and how they interrelate with the Kaiser Records Request form can enhance the patient experience and streamline communication with healthcare providers.
The Authorization for Release of Medical Records form is similar to the Medical Release Authorization form. Both documents allow patients to authorize the release of their medical information to a third party. They require specific details about the patient, including their name and date of birth, as well as the recipient’s information. Both forms also typically include a section for the purpose of the disclosure, ensuring that the patient understands why their information is being shared.
Another comparable document is the Health Information Release form. This form, like the Kaiser Records Request, is designed for patients to give consent for their health information to be disclosed. It often specifies the types of records that can be released, such as medical history or treatment records. Additionally, both forms may have a designated time frame for which the authorization is valid, ensuring that the patient’s consent is time-limited.
The Patient Authorization for Disclosure of Health Information is also similar. This document allows patients to specify which types of medical records they want to be shared. Similar to the Kaiser form, it includes options for including sensitive information, such as mental health records or substance abuse treatment. This ensures that patients can control what personal information is disclosed to third parties.
The Consent for Release of Information form shares similarities with the Kaiser Records Request form as well. Both documents require the patient to provide their personal details and specify the recipient of the records. They also include a section where patients can indicate the purpose of the release, ensuring that the information is shared for appropriate reasons.
The Release of Information Authorization form is another document that functions similarly. It allows patients to authorize the sharing of their health information with specified individuals or organizations. Like the Kaiser form, it requires the patient’s signature and often includes a revocation clause, which allows patients to cancel their authorization at any time.
The Patient Consent for Medical Records Release form is also comparable. This document is used to obtain patient consent for sharing medical records with third parties. Both forms emphasize the importance of patient understanding and consent, often requiring a signature to confirm that the patient is aware of what information is being shared and with whom.
Another related document is the Medical Records Transfer Request form. This form is used when a patient wishes to transfer their medical records from one healthcare provider to another. Similar to the Kaiser Records Request, it includes fields for patient identification and recipient details, ensuring that the transfer of information is conducted smoothly and securely.
The Authorization for Use and Disclosure of Protected Health Information form is similar in purpose and structure to the Kaiser Records Request form. Both documents require patients to authorize the release of their health information and provide specific details about the recipient. They also include sections for patients to specify the types of information to be disclosed, ensuring that only relevant records are shared.
Lastly, the Third-Party Medical Records Release form is comparable to the Kaiser Records Request. This document allows patients to authorize the release of their medical records to a designated third party. Like the Kaiser form, it includes sections for identifying the patient and the recipient, as well as specifying the purpose of the disclosure, ensuring clarity and compliance with privacy regulations.
When filling out the Kaiser Records Request form, it’s important to be thorough and accurate. Here are some key dos and don’ts to keep in mind:
When filling out the Kaiser Records Request form, consider these key takeaways to ensure a smooth process: