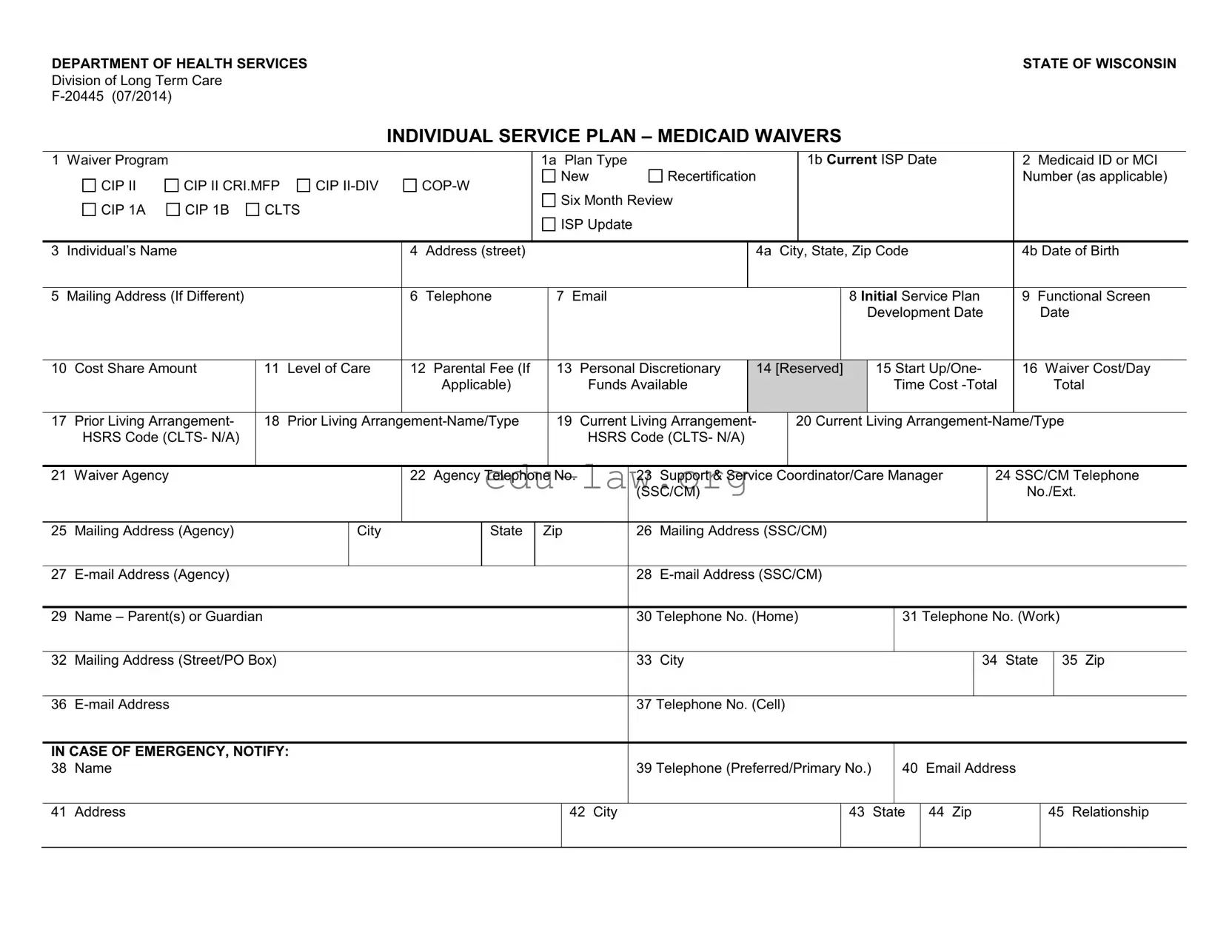
The Individual Service Plan (ISP) in Wisconsin is a crucial document designed to outline the specific needs and services required for individuals enrolled in Medicaid waiver programs. This form serves as a roadmap for care, detailing essential information such as the individual's name, address, and Medicaid ID, as well as the type of waiver program they are participating in. It includes sections for documenting the individual's living arrangements, support coordinators, and service providers, ensuring that all parties involved have a clear understanding of the care plan. Notably, the ISP emphasizes the individual's rights and choices, allowing them to select from various services and providers tailored to their unique circumstances. Regular reviews and updates of the plan are mandated to ensure that the services remain relevant and effective, fostering an environment where individuals can thrive in their chosen living situations. Furthermore, the form includes provisions for emergency contacts and verification of participant rights, reinforcing the commitment to informed decision-making and advocacy for those receiving services. In essence, the ISP not only facilitates personalized care but also empowers individuals by placing them at the center of their service planning process.

DEPARTMENT OF HEALTH SERVICESSTATE OF WISCONSIN
Division of Long Term Care
INDIVIDUAL SERVICE PLAN – MEDICAID WAIVERS
1 Waiver Program |
|
|
|
|
|
|
|
|
1a Plan Type |
|
|
|
|
|
1b Current ISP Date |
|
|
|
|
2 Medicaid ID or MCI |
|
||||||||||||
|
CIP II |
CIP II CRI.MFP |
CIP |
|
|
New |
|
Recertification |
|
|
|
|
|
|
|
|
|
|
|
|
Number (as applicable) |
|
|||||||||||
|
|
|
Six Month Review |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
CIP 1A |
CIP 1B |
CLTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
ISP Update |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
Individual’s Name |
|
|
|
|
|
4 |
Address (street) |
|
|
|
|
|
|
|
4a |
City, State, Zip Code |
|
|
|
|
|
4b Date of Birth |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5 |
Mailing Address (If Different) |
|
|
|
6 |
Telephone |
|
7 |
|
|
|
|
|
|
8 Initial Service Plan |
|
9 Functional Screen |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Development Date |
|
|
Date |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
10 |
Cost Share Amount |
|
11 |
Level of Care |
12 Parental Fee (If |
|
13 |
Personal Discretionary |
14 [Reserved] |
|
15 Start Up/One- |
|
16 Waiver Cost/Day |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
Applicable) |
|
|
|
Funds Available |
|
|
|
|
|
|
|
Time Cost |
|
|
|
Total |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
17 |
Prior Living Arrangement- |
|
18 |
Prior Living |
|
19 |
Current Living Arrangement- |
|
20 Current Living |
|
|||||||||||||||||||||||
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
21 |
Waiver Agency |
|
|
|
|
|
22 Agency Telephone |
No. |
|
23 |
Support & Service |
Coordinator/Care Manager |
|
|
24 SSC/CM Telephone |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
No./Ext. |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
25 |
Mailing Address (Agency) |
|
|
City |
|
|
State |
Zip |
|
|
26 |
Mailing Address (SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
27 |
|
|
|
|
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29 |
Name – Parent(s) or Guardian |
|
|
|
|
|
|
|
|
|
|
|
30 |
Telephone No. (Home) |
|
31 Telephone No. (Work) |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
32 |
Mailing Address (Street/PO Box) |
|
|
|
|
|
|
|
|
|
|
33 |
City |
|
|
|
|
|
|
|
|
|
|
34 |
State |
35 Zip |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
37 |
Telephone No. (Cell) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
IN CASE OF EMERGENCY, NOTIFY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
38 |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
Telephone (Preferred/Primary No.) |
|
40 |
Email Address |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
41 |
Address |
|
|
|
|
|
|
|
|
|
|
42 City |
|
|
|
|
|
43 |
|
State |
44 |
Zip |
|
|
45 Relationship |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
62 Service Code #
63 Service Name
64 |
65 |
Outcome No. |
Service Provider Name Address and |
Telephone No. |
|
|
(Email, cell phone no., if known) |
65a
Start Date
65b
End Date
66
Unit Cost ($/hr; day)
67
Authorized Units of Service and Frequency
(#/day or week or month)
68 |
69 |
Daily Cost (total |
Funding |
yearly ÷ 365 days) |
Source |
|
|

70 PARTICIPANT INFORMED – R IGHTS AND CHOICE (Review REQUIRED at initial plan development and recertification.)
I have been informed that I have a RIGHT TO CHOOSE between a nursing home or
I have been informed of my CHOICES in the waiver programs, including my right to CHOOSE the TYPE OF SERVICES I receive under my service plan.
I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.
I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made about my ELIGIBILITY to participate in the HCBS program.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made that would DENY, REDUCE OR TERMINATE the services I receive.
By my signature below I indicate I have chosen to accept community services through a Medicaid Home and Community Waiver Program.
71 UPDATE/REVIEW VERIIFICATION - APPLIES TO PLAN REVIEW OR ISP UPDATE ONLY
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.
The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
SIGNATURES: ISP Signature Requirements apply at the time of plan development, review and recertification.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Authorized Representative

CIP
A variance to the
A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
BY SIGNING BELOW, THE SUPPORT AND SERVICE COORDINATOR / CARE MANAGER ATTESTS TO THE FOLLOWING:
1.The environment is
2.The facility is the preferred residence of the applicant/participant or his/her legal representative.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Legal Representative
| Fact Name | Description |
|---|---|
| Form Purpose | The Individual Service Plan (ISP) form is used to outline the services and supports available to individuals under Medicaid Waivers in Wisconsin. |
| Governing Law | This form is governed by Wisconsin Statutes Chapter 46, which pertains to the provision of long-term care services and supports. |
| Review Frequency | Participants must undergo a six-month review of their ISP to ensure that services remain appropriate and effective. |
| Participant Rights | Individuals have the right to choose their services and providers, as well as the right to request a hearing if they disagree with eligibility or service decisions. |
Completing the Individual Service Plan (ISP) Wisconsin form is a crucial step in ensuring that individuals receive the appropriate services and supports they need. Following the steps outlined below will help streamline the process and ensure that all necessary information is accurately captured.
What is the Individual Service Plan (ISP) Wisconsin form?
The Individual Service Plan (ISP) Wisconsin form is a document used to outline the services and supports needed for individuals enrolled in Medicaid waiver programs. It details the participant's needs, preferences, and the services they will receive to ensure their well-being and quality of life.
Who needs to complete the ISP form?
The ISP form must be completed for individuals who are applying for or are already enrolled in Medicaid Home and Community-Based Services (HCBS) programs. This includes participants in various waiver programs, such as CIP II, CLTS, and others.
What information is required on the ISP form?
The ISP form requires detailed information, including the individual's name, address, Medicaid ID, date of birth, current living arrangements, and contact information for the participant and their support coordinator. It also includes specific service codes, service providers, and details about the services being provided.
How often should the ISP be reviewed?
The ISP should be reviewed at least every six months. During this review, the participant or their guardian will discuss any changes in needs or services. If updates are necessary, they will be documented on the form.
What rights do participants have regarding their ISP?
Participants have the right to choose between various service options, including community services or institutional care. They can select from qualified providers and are informed of their rights and responsibilities within the Medicaid waiver programs. Participants also have the right to request a hearing if they disagree with decisions regarding their eligibility or services.
What happens if changes are needed in the ISP?
If changes are required, the support coordinator will work with the participant or guardian to update the ISP. This may involve adding, reducing, or changing the frequency of services. The updated information will be documented on the ISP form.
Who signs the ISP form?
The ISP form must be signed by the participant, their guardian or authorized representative, and the support and service coordinator. Witness signatures may also be required. These signatures indicate agreement with the content of the plan and the services to be provided.
What is the purpose of the cost share amount listed on the ISP?
The cost share amount reflects any financial contribution that the participant may need to make toward their care. This amount is determined based on the individual’s financial situation and is included in the ISP to ensure transparency regarding funding for services.
Where is the completed ISP form submitted?
The completed ISP form is submitted to the Department of Health Services (DHS) and copies are provided to the county care manager or support coordinator, the individual, and their authorized representative. This ensures that all parties involved have access to the most current service plan.
Incomplete Personal Information: Failing to provide all required personal details, such as the individual's name, address, and date of birth, can lead to delays in processing the form.
Incorrect Medicaid ID: Entering an incorrect Medicaid ID or MCI number can result in significant issues with eligibility verification.
Missing Signatures: Not obtaining all necessary signatures, including those of the participant, guardian, and care manager, can invalidate the form.
Omitting Service Details: Failing to specify the services required, including start and end dates, can lead to confusion and unmet needs.
Ignoring Cost Share Information: Neglecting to fill out the cost share amount can complicate financial assessments and service delivery.
Not Updating Changes: Failing to document changes during six-month reviews can result in outdated service plans that do not reflect current needs.
Inaccurate Emergency Contact Information: Providing incorrect or outdated emergency contact details may hinder timely assistance in critical situations.
Neglecting Participant Rights: Not reviewing or acknowledging the participant's rights and choices can lead to misunderstandings about their options.
Ignoring Agency Information: Omitting or incorrectly entering the waiver agency's contact information can delay communication and support.
The Individual Service Plan (ISP) Wisconsin form is a vital document used in the Medicaid waiver process to outline the services and supports an individual requires. Alongside this form, several other documents are commonly utilized to ensure a comprehensive approach to service delivery. Each of these documents plays a crucial role in supporting the individual’s needs and preferences.
Each of these documents complements the Individual Service Plan, creating a robust framework for delivering personalized care. Together, they ensure that individuals receive the support they need while respecting their rights and preferences.
The Individualized Education Program (IEP) is a document similar to the Individual Service Plan in Wisconsin. It is specifically designed for children with disabilities and outlines the educational goals and services that will be provided to support their learning. Like the Individual Service Plan, the IEP is developed collaboratively with input from parents, teachers, and specialists. Both documents emphasize the importance of tailoring services to meet the unique needs of the individual, ensuring that they receive appropriate support in their respective environments.
The Personal Support Plan (PSP) also shares similarities with the Individual Service Plan. The PSP is often used for individuals with developmental disabilities and focuses on enhancing their quality of life through personalized support. Both plans involve a comprehensive assessment of the individual's needs and preferences, and they serve as a roadmap for the services and supports required. The collaborative approach in both documents ensures that the individual's voice is heard and prioritized in the planning process.
The Service Plan for Home and Community-Based Services (HCBS) is another document akin to the Individual Service Plan. This plan is tailored for individuals who require assistance in their homes or community settings due to disabilities or health concerns. Like the Individual Service Plan, the HCBS Service Plan outlines specific services, goals, and support strategies, emphasizing the individual's right to choose their preferred services and providers. Both documents aim to promote independence and enhance the individual's ability to live in the community.
The Comprehensive Assessment and Service Planning (CASP) document is also comparable to the Individual Service Plan. The CASP is utilized in various healthcare settings to assess an individual's needs comprehensively. It includes input from healthcare providers, family members, and the individual themselves. Similar to the Individual Service Plan, the CASP focuses on identifying strengths and challenges, guiding the development of a tailored support plan that addresses the individual's unique circumstances.
The Treatment Plan, commonly used in mental health services, bears resemblance to the Individual Service Plan as well. It outlines the therapeutic goals and interventions for individuals receiving mental health support. Both documents are developed collaboratively, with input from the individual and their support team. They share the common goal of providing targeted services that promote recovery and well-being, ensuring that the individual's needs and preferences are central to the planning process.
Finally, the Individualized Family Service Plan (IFSP) is another document similar to the Individual Service Plan. The IFSP is specifically designed for infants and toddlers with developmental delays and their families. It focuses on the child's developmental needs and the family's resources and supports. Like the Individual Service Plan, the IFSP emphasizes collaboration among family members and service providers, ensuring that the child's needs are met holistically and that the family is actively involved in the planning and implementation of services.
When filling out the Individual Service Plan (ISP) Wisconsin form, it is essential to follow specific guidelines to ensure accuracy and compliance. Below are key actions to take and avoid:
Misconceptions about the Individual Service Plan (ISP) Wisconsin form can lead to confusion regarding its purpose and function. The following are six common misconceptions:
Filling out the Individual Service Plan (ISP) Wisconsin form is an important step in accessing Medicaid waiver services. Here are some key takeaways to keep in mind:
By keeping these points in mind, individuals and their families can navigate the ISP process more effectively, ensuring access to the necessary services and supports.