The Home Health Audit form serves as a comprehensive tool designed to ensure that home health agencies comply with regulatory requirements and maintain high standards of patient care. This form encompasses various critical components that assess the quality and completeness of medical records. It includes sections for evaluating patient admission processes, such as the timely initiation of care and the completion of necessary documentation, like the Patient Referral Sheet and the Pre-Admit Physician Order. Additionally, the form requires auditors to verify that diagnoses are accurately recorded and supported by appropriate medical necessity. It emphasizes the importance of signed agreements, consent forms, and acknowledgment of patient rights. The audit also addresses the ongoing management of patient care, including documentation of skilled nursing visits, therapy evaluations, and medication profiles. Each element is designed to capture essential information that reflects compliance with agency policies and ensures that patient needs are met effectively. Moreover, the form incorporates measures for assessing care quality, such as pain assessments and fall risk evaluations, which are crucial for enhancing patient safety and outcomes. Ultimately, the Home Health Audit form is an essential instrument for maintaining accountability and improving the quality of home health services.
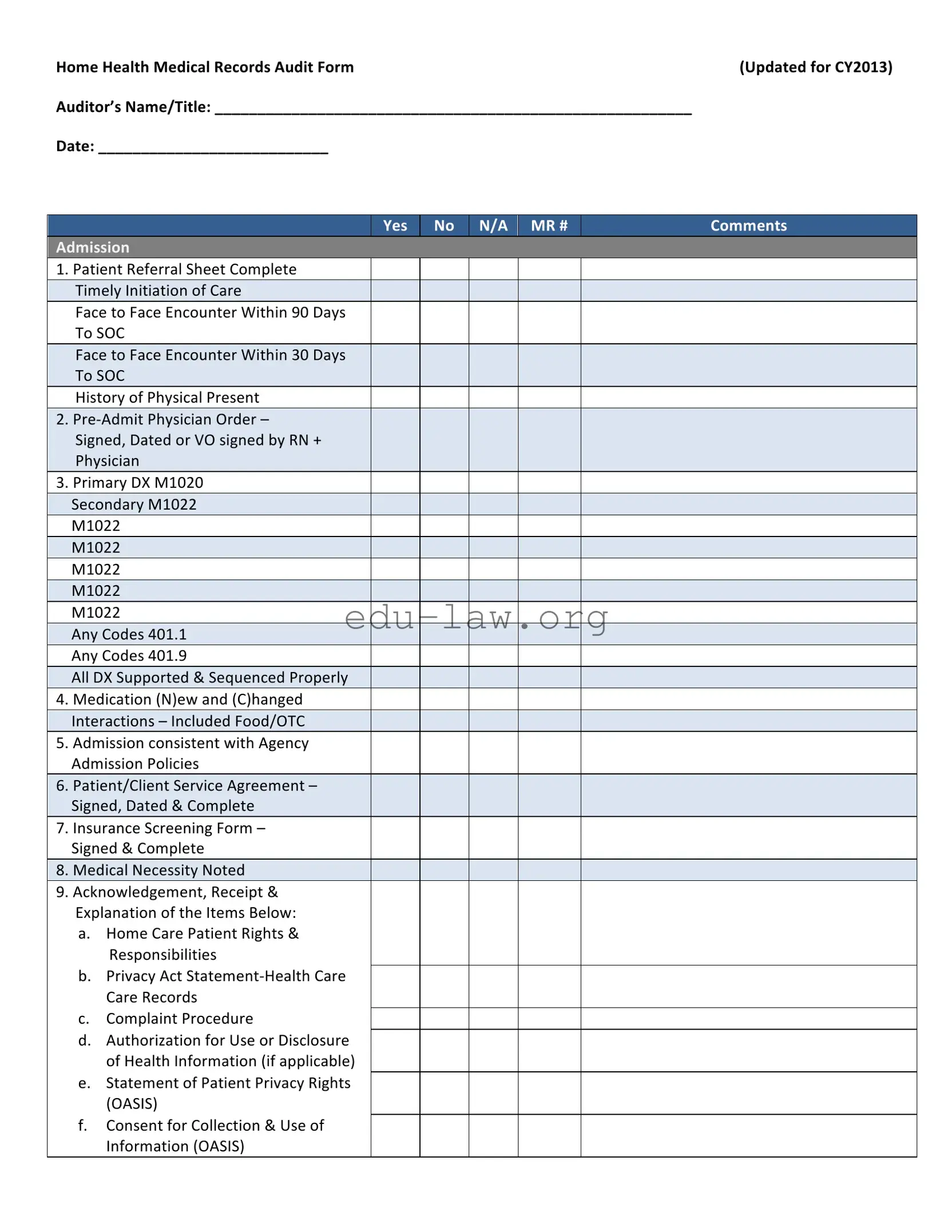
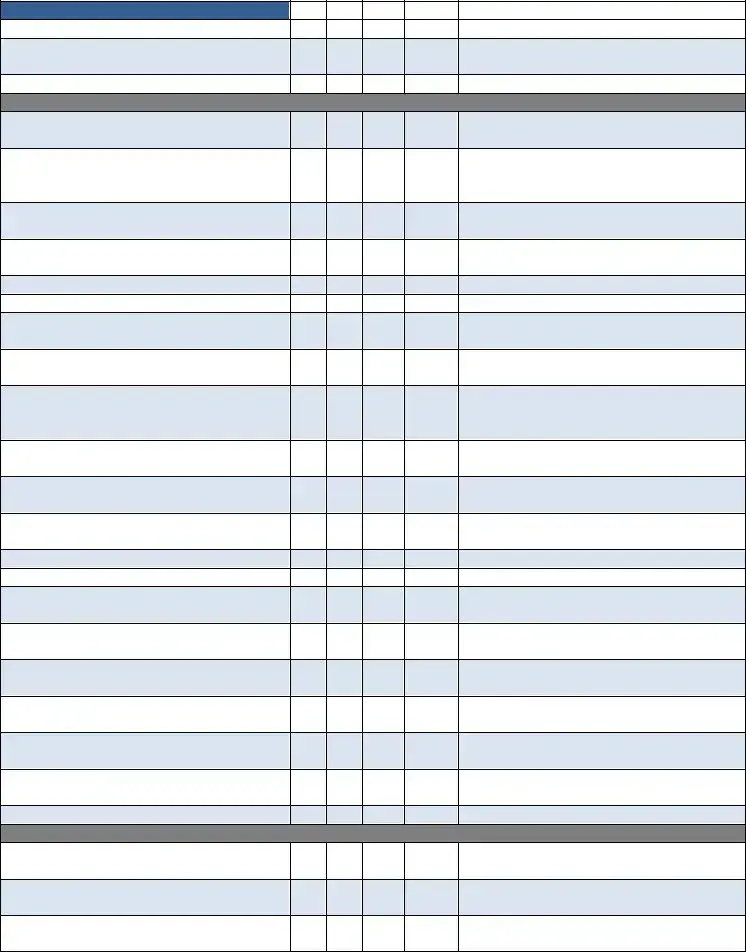
Home Health Medical Records Audit Form |
(Updated for CY2013) |
Auditor’s Name/Title: ________________________________________________________ |
|
Date: ___________________________ |
|
Yes
No
N/A MR #
Comments
Admission
1.Patient Referral Sheet Complete Timely Initiation of Care
Face to Face Encounter Within 90 Days To SOC
Face to Face Encounter Within 30 Days To SOC
History of Physical Present
2.Pre‐Admit Physician Order –
Signed, Dated or VO signed by RN + Physician
3.Primary DX M1020 Secondary M1022 M1022
M1022
M1022
M1022
M1022
Any Codes 401.1 Any Codes 401.9
All DX Supported & Sequenced Properly
4.Medication (N)ew and (C)hanged Interactions – Included Food/OTC
5.Admission consistent with Agency Admission Policies
6.Patient/Client Service Agreement – Signed, Dated & Complete
7.Insurance Screening Form – Signed & Complete
8.Medical Necessity Noted
9.Acknowledgement, Receipt & Explanation of the Items Below:
a.Home Care Patient Rights & Responsibilities
b.Privacy Act Statement‐Health Care Care Records
c.Complaint Procedure
d.Authorization for Use or Disclosure of Health Information (if applicable)
e.Statement of Patient Privacy Rights (OASIS)
f.Consent for Collection & Use of Information (OASIS)
Yes |
No |
N/A |
MR # |
Comments |
|
|
|
|
|
g.Emergency Preparedness Plan/Safety Instructions
h.Advance Directives & HHABN
10. Complete Post Evaluation –
D/C Summary Report by RN/PT/OT/ST on:
a. Start of Care
b. Resumption of Care
c. Recertification
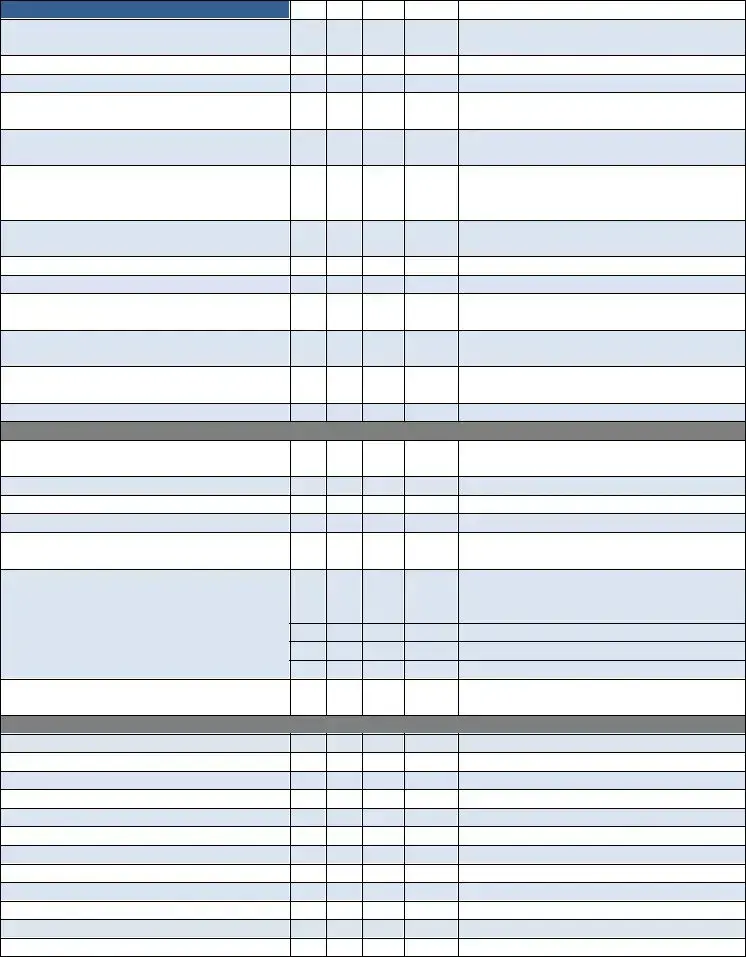
Plan of Care 485
11.Plan of Care Signed & Dated by Physician Within 30 Working Days or State Specific days‐ ________
12.Diagnoses Consistent with Care Ordered
13.Orders Current
14. Focus of Care Substantiated
15.Daily Skilled Nurse Visit Frequencies with Indication of End Point
16. Measurable Goals for Each Discipline
17. Tinetti or TUG Completed at SOC
18. Recertification Plan of Care Signed &
Dated Within 30 Days or State Required
Time
19.BiD Insulin Visits Documented with Vision, Musculoskeletal Need, Not Willing/Capable Caregiver. MSW Every Episode
20. Skilled Nurse Consult
Medication Profile Sheet
21.Medication Profile Consistent with the 4 485
22. Medication Profile Updated at
Recertification, ROC, SCIC, Initialed &
Dated
23.Medication Profile Complete with Pharmacy Information
Physician Orders/Change Verbal Orders
24. Change/Verbal Orders Include Disciplines, Goals, Frequencies, Reason for Change, Additional Supplies as Appropriate
25.Change Orders Signed & Dated by Physician Within 30 Working Days
OASIS Assessment Form
26. Complete, Signed & Dated by:
___________________________
27.M2200 Answer Meets the Threshold for a Medicare High Case Mix Group
28. M1020 & M1022 Diagnoses & ICD‐9 are Consistent with the Plan of Care
Yes |
No |
N/A |
MR # |
Comments |
|
|
|
|
|
29.All OASIS Assessments Were Exported Within 30 Days
30. OASIS Recertifications Were Done
Within 5 Days of the End of the Episode
31.All OASIS Were Reviewed for Consistency in Coordination with the Discipline Who Completed the Form
Skilled Nursing Clinical Notes
32. Visit Frequencies & Duration are Consistent with Physician Orders
33.Orders Written for Visit Frequencies/ Treatment Change
34. Homebound Status Supported on Each Visit Note
35.Measurable Goals for Each Discipline with Specific Time Frames
36. Frequency of Visits Appropriate for Patient’s Needs & Interventions Provided
37. Appropriate Missed Visit (MV) Notes
38. Skilled Care Evident on Each Note
39. Evidence of Coordination of Care
40. Every Note Signed & Dated
41. Follows the Plan of Care (485)
42. Weekly Wound Reports are Completed
43. Missed Visit Reports are Completed
44. Pain Assessment Done Every Visit with Intervention (If Applicable)
45.Abnormal Vital Signs Reported to Physician & Case Managers
46. Evidence of Interventions with Abnormal Parameters/Findings
47.Skilled Nurse Discharge Summary/ Instructions Completed
48. LVN Supervisory Visit Every 30 Days by Registered Nurse
Certified Home Health Aide
49.Visit Frequencies & Duration Consistent with Physician Orders
50. Personal Care Instructions Documented,
Signed & Dated
51.Personal Care Instructions Modified as Appropriate
52. Notes Consistent with Personal Care Instructions Noted on the CHHA Assignment Sheet Completed by the RN/PT/ST/OT
53.Notes Reflect Supervisor Notification of Patient Complications or Changes
54. Visit Frequencies Appropriate for Patient Needs
Yes |
No |
N/A |
MR # |
Comments |
|
|
|
|
|
55. Each Note Reflects Personal Care Given
56. Supervisory Visits at Least Every 14 Days by RN or PT
57. Every Note Signed & Dated
PT
58. Assessment Includes Evaluation,
Care Plan & Visit Note
59.Evaluation Done Within 48 Hours of Referral Physician Order or Date Ordered
60. Visit Frequencies/Duration Consistent with Physician Orders
61.Evidence of Need for Therapy/Social Service
62. Appropriate Missed Visit (MV) Notes
63. Notes Consistent with Physician Orders
64. Evidence of Skilled Service(s) Provided
in Each Note
65.Treatment/Services Provided Consistent with Physician Orders & Care Plan
66. Notes Reflect Supervisor & Physician Notification of Patient Complications or Changes
67.Specific Evaluation & “TREAT” Orders Prior to Care
68. Verbal Orders for “TREAT” Orders Prior to Care
69.Homebound Status Validated in Each Visit Note
70. Notes Reflect Progress Toward Goals
71. Evidence of Discharge Planning
72. Evidence of Therapy Home Exercise
Program
73.Discharge/Transfer Summary Complete with Goals Met/Unmet
74. Assessment & Evaluation performed by Qualified Therapist Every 30 Days
75.Supervision of PTA/OTA at Least Every 2 Weeks
76. Qualified Therapy Visit 13th Visit (11, 12, 13)
77.Qualified Therapy Visit 19th Visit (17, 18, 19)
78. Every Visit Note Signed & Dated
SLP
79.Assessment Includes Evaluation, Care Plan & Visit Note
80. Evaluation Done Within 48 Hours of Referral Physician Order or Date Ordered
81.Visit Frequencies/Duration Consistent with Physician Orders
Yes |
No |
N/A |
MR # |
Comments |
|
|
|
|
|
82. Evidence of Need for Therapy/Social Service
83. Appropriate Missed Visit (MV) Note
84. Notes Consistent with Physician Orders
85.Evidence of Skilled Service(s) Provided in Each Note
86. Treatment/Services Provided Consistent with Physician Orders & Care Plan
87.Notes Reflect Supervisor & Physician Notification of Patient Complications or Changes
88. Homebound Status Validated in Each Visit
Note
89. Notes Reflect Progress Toward Goals
90. Evidence of Discharge Planning
91.Evidence of Therapy Home Exercise Program
92. Discharge/Transfer Summary Complete with Goals Met/Unmet
93.Supervision of PTA/OTA at Least Every 2 Weeks
94. Every Visit Note Signed & Dated
Miscellaneous
95.Progress Summary Completed(30‐45Days) Each Episode Signed & Dated
96. Field Notes are Submitted & Complete
97. Chart in Chronological Order
98. Chart in Order per Agency Policy
99.Patient Name & Medical Records Number on Every Page
100. Physician Orders are Completed/ Updated for Clinical Tests Such as:
a. Coumadin: Protime/INR
b. Hemoglobin A1C
c. CBC, Metabolic Panel, CMP
d. Others: _______________________
101.Communication with Physician Regarding Test Results
Process Measures:
Timely Initiation of Care
Influenza Received
PPV Ever Received
Heart Failure
DM Foot Care & Education
Pain Assessment
Pain Intervention
Depression Assessment
Medication Education
Falls Risk Assessment
Pressure Ulcer Prevention
Pressure Ulcer Risk Assessment
Additional Comments/Recommendations ‐
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
THE FOLLOWING IS APPLICABLE FOR QUARTERLY MEDICAL REVIEW REPORT
REVIEWED AND SIGNED BY THE FOLLOWING DISCIPLINARY REPRESENTATIVE
______________________________________ |
______________________________________ |
Registered Nurse |
Occupational Therapist (If Applicable) |
______________________________________ |
______________________________________ |
Physical Therapist (If Applicable) |
Speech Language Pathologist (If Applicable) |
______________________________________ |
______________________________________ |
Medical Director |
MSW (If Applicable) |
MR # ______________________
| Fact Name | Details |
|---|---|
| Form Title | Home Health Medical Records Audit Form (Updated for CY2013) |
| Purpose | This form is used to evaluate compliance with home health care regulations and agency policies. |
| Key Components | The audit covers various aspects such as patient admission, medical necessity, care plans, and skilled nursing documentation. |
| Signature Requirements | Multiple sections require signatures and dates from healthcare professionals, including physicians and registered nurses. |
| State-Specific Regulations | Regulations may vary by state. For example, California requires the Plan of Care to be signed within 30 days. |
| Data Export Timeline | All OASIS assessments must be exported within 30 days of completion to ensure timely reporting and compliance. |
Filling out the Home Health Audit form is an essential step in ensuring compliance and maintaining high standards of care. By following the steps outlined below, you can complete the form accurately and efficiently.
What is the purpose of the Home Health Audit form?
The Home Health Audit form is designed to evaluate the quality and compliance of home health care services. It assesses various aspects of patient care, including documentation accuracy, adherence to care plans, and the timely execution of services. By using this form, agencies can ensure they meet regulatory requirements and provide high-quality care to their patients.
Who should complete the Home Health Audit form?
The Home Health Audit form should be completed by qualified auditors, typically individuals with experience in home health care operations. This may include registered nurses, compliance officers, or other healthcare professionals trained in auditing practices. Their expertise ensures that the audit is thorough and that any potential issues are identified and addressed.
How often should the Home Health Audit form be used?
What are the key components assessed in the Home Health Audit form?
Key components assessed in the Home Health Audit form include patient admission procedures, physician orders, medication management, and documentation of skilled nursing visits. The form evaluates whether all required signatures are present, if care plans are updated, and if patient rights and responsibilities are communicated effectively. Each section is crucial for ensuring that care is delivered safely and in accordance with established guidelines.
Failing to complete the patient referral sheet accurately. This is a crucial document that sets the stage for the entire care process.
Not signing or dating the pre-admit physician order. This oversight can lead to significant delays in care initiation.
Inadequate documentation of medication interactions. It’s essential to include all relevant interactions, including food and over-the-counter medications.
Neglecting to ensure that the patient/client service agreement is signed and complete. This document is vital for establishing clear expectations between the agency and the patient.
Overlooking the acknowledgment of patient rights and responsibilities. Patients must be informed of their rights to ensure they receive appropriate care.
Failing to document skilled nurse visit frequencies accurately. This information is necessary to ensure that care meets the patient’s needs.
Not providing measurable goals for each discipline. Goals must be specific to track progress effectively and adjust care as needed.
Forgetting to include patient name and medical record number on every page of the audit form. This simple step is crucial for maintaining accurate and organized records.
In the realm of home health care, various forms and documents are essential for ensuring compliance, quality of care, and proper documentation. These documents work in conjunction with the Home Health Audit form to provide a comprehensive overview of patient care and agency practices. Below are several key forms that are commonly utilized alongside the Home Health Audit form.
Each of these documents plays a vital role in the home health care process, contributing to effective communication, quality assurance, and compliance with regulatory requirements. By maintaining accurate and comprehensive documentation, agencies can enhance patient outcomes and foster a culture of accountability and excellence in care.
The Home Health Medical Records Audit Form shares similarities with the Patient Care Plan. Both documents focus on documenting the care provided to patients and ensuring that all necessary steps are taken to meet their needs. The Patient Care Plan outlines specific goals, interventions, and the responsibilities of healthcare providers, just like the Home Health Audit form emphasizes the importance of compliance with care protocols and documentation requirements. Both forms aim to ensure that patients receive consistent and high-quality care throughout their treatment.
Another document that aligns closely with the Home Health Audit form is the Quality Assurance Performance Improvement (QAPI) Plan. This plan is designed to monitor and improve the quality of care provided in home health settings. Similar to the Home Health Audit form, the QAPI Plan includes measures for evaluating patient outcomes, adherence to protocols, and staff performance. Both documents emphasize the importance of continuous improvement and accountability in delivering home health services.
The Plan of Care document is also comparable to the Home Health Audit form. The Plan of Care outlines the specific treatments and services a patient will receive, ensuring that all healthcare providers are on the same page. Both documents require signatures and dates from healthcare professionals to confirm that the care plan is understood and agreed upon. This ensures that all actions taken align with the patient's needs and the overall goals of their treatment.
Similarly, the OASIS Assessment Form is another document that shares a common purpose with the Home Health Audit form. OASIS assessments collect essential data about a patient's health status and care needs. Like the Home Health Audit form, OASIS assessments require timely completion and accuracy to ensure that care is appropriate and effective. Both documents are vital for compliance with regulations and for maintaining high standards of care.
The Skilled Nursing Clinical Notes are also akin to the Home Health Audit form. These notes provide detailed accounts of the services delivered during each visit, similar to how the audit form tracks compliance and care delivery. Both documents require documentation of patient interactions, interventions, and any changes in the patient's condition. This ensures that all care provided is recorded and can be reviewed for quality assurance purposes.
Another document that bears resemblance to the Home Health Audit form is the Patient Rights and Responsibilities document. This document outlines the rights of patients receiving home health care, ensuring they are informed and protected. Both the Patient Rights document and the Home Health Audit form aim to uphold patient dignity and safety while providing care. They serve as reminders of the ethical obligations healthcare providers have toward their patients.
Finally, the Discharge Summary is similar to the Home Health Audit form in that it documents the patient's progress and the outcomes of their care. The Discharge Summary includes information about the patient's condition at the time of discharge and any follow-up care needed. Like the Home Health Audit form, it emphasizes the importance of thorough documentation and communication among healthcare providers to ensure continuity of care as patients transition out of home health services.
When filling out the Home Health Audit form, consider the following guidelines:
Misconception 1: The Home Health Audit form is only for billing purposes.
This form serves a broader purpose. It ensures compliance with care standards, evaluates the quality of services, and helps maintain patient safety.
Misconception 2: All items on the form must be completed for every patient.
Not every section applies to all patients. Some items may be marked as N/A (not applicable) depending on individual circumstances.
Misconception 3: The form is only relevant for initial admissions.
The Home Health Audit form is used throughout the patient's care, including recertifications and discharges, ensuring ongoing compliance and quality.
Misconception 4: Completing the form is a one-time task.
Regular updates are necessary. The form must be revisited and updated as patient needs change or as new information becomes available.
Misconception 5: Only nurses need to complete the Home Health Audit form.
While nurses play a significant role, other healthcare professionals, such as therapists and social workers, also contribute to the audit process.
Misconception 6: The audit form is not important for patient care.
This form directly impacts patient care quality. It identifies areas for improvement, ensuring that patients receive the best possible services.
Misconception 7: The Home Health Audit form is the same across all agencies.
Different agencies may have unique requirements. While the core elements remain similar, specific items can vary based on agency policies and state regulations.
When using the Home Health Audit form, several key points should be kept in mind to ensure accuracy and compliance. Here are the essential takeaways: