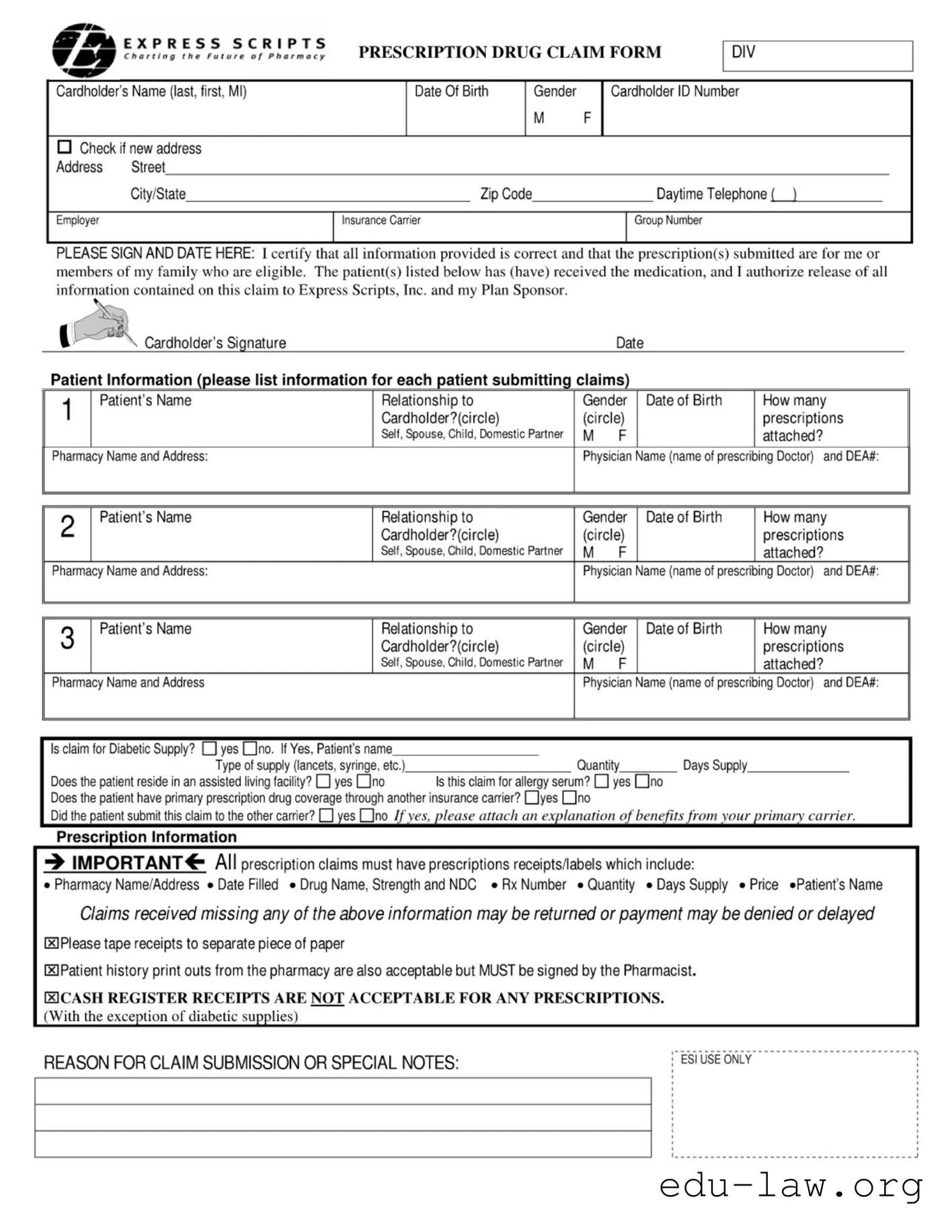
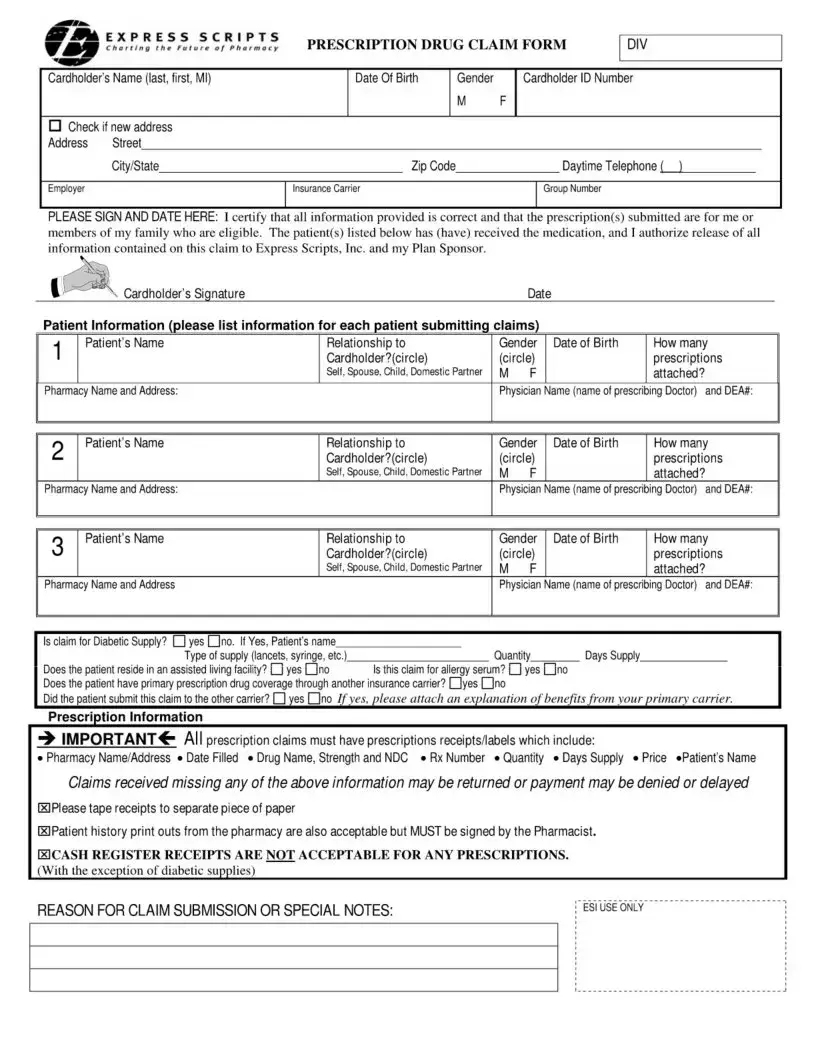
The Express Scripts Fax form is a vital tool for managing prescription drug claims. It streamlines the process for cardholders seeking reimbursement for their medications. Key sections of the form include personal information about the cardholder, such as their name, address, and insurance details. Each family member submitting claims must be listed, along with their relationship to the cardholder and details about their prescriptions. The form requires specific information about the medications, including pharmacy details, prescribing physician, and necessary receipts. It’s important to ensure all required information is complete, as missing data can lead to delays or denials in processing claims. Additionally, the form includes a section for any special notes, allowing cardholders to provide further context if needed. Properly completing this form can significantly ease the claims process and help ensure timely reimbursement for prescription costs.
сЛГЛ E ?Л.?« СДІЛЛ S |
PRESCRIPTION DRUG CLAIM FORM |
||
Cardholder’s Name (last, first, Ml) |
Date Of Birth |
Gender |
Cardholder ID Number |
|
|
M |
F |
Check if new address |
|
|
|
Address Street |
|
|
|
Citv/State |
Zip Code |
|
Davtime Telephone ( ) |
Employer |
Insurance Carrier |
|
Group Number |
PLEASE SIGN AND DATE HERE: I certify that all information provided is correct and that the prescription(s) submitted are for me or members of my family who are eligible. The patient(s) listed below has (have) received the medication, and I authorize release of all information contained on this claim to Express Scripts, Inc. and my Plan Sponsor.
Cardholder’s Signature |
Date |
Patient Information (please list information For each patient submitting claims)
1 |
Patient’s Name |
Relationship to |
Gender Date of Birth |
How many |
|
|
Cardholder?(circle) |
(circle) |
prescriptions |
||
|
|
Self, Spouse, Child, Domestic Partner |
M |
F |
attached? |
Pharmacy Name and Address: |
|
Physician Name (name of prescribing Doctor) and DEA#: |
|||
2 |
Patient’s Name |
Relationship to |
|
Cardholder?(circle) |
|
|
|
Self, Spouse, Child, Domestic Partner |
Pharmacy Name and Address: |
|
|
3 |
Patient's Name |
Relationship to |
|
Cardholder?(circle) |
|
Self, Spouse, Child, Domestic Partner
Pharmacy Name and Address
Gender Date of Birth |
How many |
|
(circle) |
prescriptions |
|
M |
F |
attached? |
Physician Name (name of prescribing Doctor) and DEA#:
Gender Date of Birth |
How many |
|
(circle) |
prescriptions |
|
M |
F |
attached? |
Physician Name (name of prescribing Doctor) and DEA#:
Is claim for Diabetic Supply? □yesdno. If Yes, Patient's name |
|
|
|
|
Type of supply (lancets, syringe, etc.) |
Quantity |
Days Supply |
||
Does the patient reside in an assisted living facility? |
yes EJno |
Is this claim for allergy serum? |
yes dno |
|
Does the patient have primary prescription drug coverage through another insurance carrier? dyes dno
Prescription Information
■» IMPORTANT^- All prescription claims must have prescriptions receipts/labels which include:
• Pharmacy Name/Address • Date Filled • Drug Name, Strength and NDC • Rx Number • Quantity • Days Supply • Price «Patient’s Name
Claims received missing any of the above information may be returned or payment may be denied or delayed
ИPlease tape receipts to separate piece of paper
(3 Patient history print outs from the pharmacy are also acceptable but MUST be signed by the Pharmacist.
ECASH REGISTER RECEIPTS ARE NOT ACCEPTABLE FOR ANY PRESCRIPTIONS.
(With the exception of diabetic supplies)
REASON FOR CLAIM SUBMISSION OR SPECIAL NOTES: |
L esi Use only |
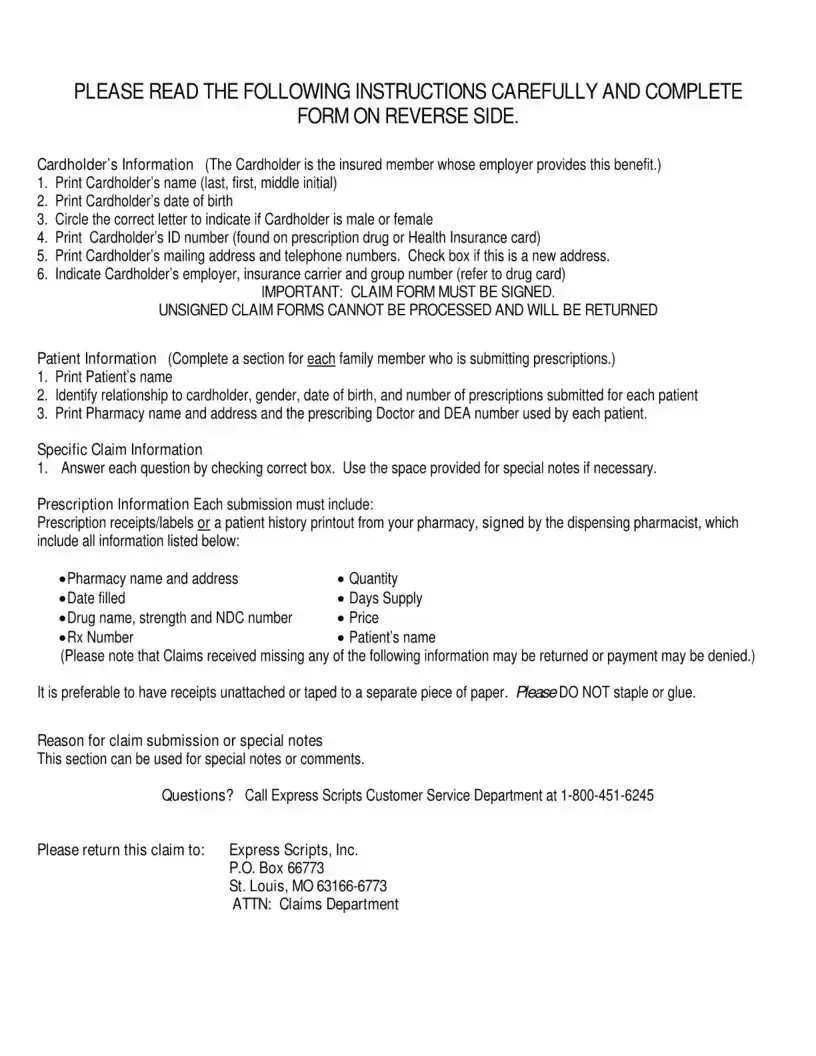
PLEASE READ THE FOLLOWING INSTRUCTIONS CAREFULLY AND COMPLETE
FORM ON REVERSE SIDE.
Cardholder’s Information (The Cardholder is the insured member whose employer provides this benefit.)
1.Print Cardholder's name (last, first, middle initial)
2.Print Cardholder’s date of birth
3.Circle the correct letter to indicate if Cardholder is male or female
4.Print Cardholder’s ID number (found on prescription drug or Health Insurance card)
5.Print Cardholder’s mailing address and telephone numbers. Check box if this is a new address.
6.Indicate Cardholder's employer, insurance carrier and group number (refer to drug card)
IMPORTANT: CLAIM FORM MUST BE SIGNED.
UNSIGNED CLAIM FORMS CANNOT BE PROCESSED AND WILL BE RETURNED
Patient Information (Complete a section for each family member who is submitting prescriptions.)
1.Print Patient’s name
2.Identify relationship to cardholder, gender, date of birth, and number of prescriptions submitted for each patient
3.Print Pharmacy name and address and the prescribing Doctor and DEA number used by each patient.
Specific Claim Information
1.Answer each question by checking correct box. Use the space provided for special notes if necessary.
Prescription Information Each submission must include:
Prescription receipts/labels or a patient history printout from your pharmacy, signed by the dispensing pharmacist, which include all information listed below:
• Pharmacy name and address |
• Quantity |
• Date filled |
«Days Supply |
• Drug name, strength and NDC number |
• Price |
• Rx Number |
• Patient's name |
(Please note that Claims received missing any of the following information may be returned or payment may be denied.)
It is preferable to have receipts unattached or taped to a separate piece of paper. HeaseDO NOT staple or glue.
Reason for claim submission or special notes
This section can be used for special notes or comments.
Questions? Call Express Scripts Customer Service Department at 1
Please return this claim to: |
Express Scripts, Inc. |
|
P.O. Box 66773 |
|
St. Louis, MO |
|
ATTN: Claims Department |
| Fact Name | Description |
|---|---|
| Cardholder Information | The form requires detailed cardholder information, including name, date of birth, gender, ID number, address, and employer information. |
| Patient Information | Each patient submitting a claim must have their information listed, including their relationship to the cardholder, gender, date of birth, and the number of prescriptions attached. |
| Prescription Requirements | All claims must include prescription receipts or labels with specific details such as pharmacy name, date filled, drug name, and price. Missing information may lead to claim denial or delays. |
| Signature Requirement | The cardholder must sign and date the form to certify that all information is correct. Unsigned forms cannot be processed. |
| Claim Submission | Claims should be mailed to Express Scripts, Inc. at the designated address. Ensure all sections of the form are completed to avoid processing issues. |
| State-Specific Laws | Different states may have specific regulations governing prescription drug claims. It is important to check local laws for compliance. |
After completing the Express Scripts Fax form, you will need to submit it along with any required documentation to ensure your claim is processed efficiently. Follow the steps below to fill out the form correctly.
For each patient submitting claims, complete the following:
Answer any specific claim questions by checking the appropriate boxes. Use the space for special notes if necessary. Make sure to include all required prescription receipts or labels with the submission.
Finally, ensure that the completed form is sent to the address provided on the form for processing.
What is the purpose of the Express Scripts Fax form?
The Express Scripts Fax form is designed to help individuals submit claims for prescription drug reimbursements. When you fill out this form, you provide essential information about yourself, your prescriptions, and your pharmacy. This allows Express Scripts to process your claim efficiently and ensure you receive the reimbursement you are entitled to for your medications.
What information do I need to provide on the form?
When completing the form, you must include several key details. Start with your personal information, such as your name, address, and contact number. You will also need to provide your cardholder ID number and details about your insurance carrier. For each patient whose prescriptions you are submitting, include their name, relationship to you, gender, date of birth, and the number of prescriptions attached. Additionally, include the pharmacy's name and address, along with the prescribing doctor's name and DEA number. Make sure to attach the necessary prescription receipts or labels, as claims missing this information may be delayed or denied.
What should I do if I have multiple prescriptions to submit?
If you have multiple prescriptions, the form allows you to list each patient separately. For each patient, fill out the required information in the designated sections. Be sure to specify the number of prescriptions attached for each individual. This ensures that Express Scripts can accurately process each claim. Remember, each submission must include the corresponding receipts or labels for all prescriptions to avoid any issues with your claim.
How do I submit the completed form?
Once you have filled out the Express Scripts Fax form and attached all necessary documentation, you can submit it by faxing it to the designated number or mailing it to the address provided on the form. If you choose to mail it, send it to Express Scripts, Inc., P.O. Box 66773, St. Louis, MO 63166-6773, and ensure that it is addressed to the Claims Department. If you have any questions during the process, you can contact Express Scripts Customer Service at 1-800-451-6245 for assistance.
Incomplete Patient Information: Failing to provide complete details for each patient can lead to delays. Each section must include the patient's name, relationship to the cardholder, gender, date of birth, and the number of prescriptions submitted.
Missing Cardholder Signature: An unsigned claim form cannot be processed. Always ensure the cardholder signs and dates the form before submission.
Incorrect Pharmacy Information: Providing inaccurate pharmacy names or addresses can result in claim denial. Double-check that the pharmacy details match the receipts.
Failure to Include Prescription Receipts: Claims must include prescription receipts or labels that contain essential information. Omitting any required details can lead to delays or denials.
Not Following Submission Guidelines: Claims that do not adhere to submission instructions, such as stapling or gluing receipts, may be returned. Always tape receipts to a separate piece of paper instead.
Ignoring Additional Coverage: If the patient has primary prescription drug coverage through another insurance carrier, this must be disclosed. Failing to do so can complicate the claims process.
When submitting claims using the Express Scripts Fax form, several additional documents may be required to ensure a smooth processing experience. Each of these documents serves a specific purpose and helps to provide the necessary information for your claim. Below is a list of commonly used forms and documents that you may encounter in conjunction with the Express Scripts Fax form.
Having these documents ready can significantly streamline the claims process. It is always advisable to double-check that all required information is included to avoid any potential issues. If you have questions or need assistance, reaching out to customer service can provide clarity and support.
The Express Scripts Fax form shares similarities with the Health Insurance Claim Form (CMS-1500). Both documents serve the purpose of submitting claims for reimbursement of medical expenses. The CMS-1500 form requires detailed patient information, including the patient’s name, date of birth, and insurance details, just like the Express Scripts form. Additionally, both forms require the signature of the claimant to certify that the information provided is accurate, ensuring that the claims process is legitimate and accountable.
Another document that resembles the Express Scripts Fax form is the Pharmacy Claim Form. This form is specifically designed for patients seeking reimbursement for prescription medications. Like the Express Scripts form, it requires patient identification, details about the prescribed medications, and the pharmacy's information. Both forms emphasize the necessity of including supporting documents, such as prescription receipts, to validate the claim being submitted.
The Patient Information Form is also similar to the Express Scripts Fax form. This document collects essential information about the patient, including their relationship to the cardholder, gender, and date of birth. The Express Scripts form includes a section for multiple patients, which is akin to how the Patient Information Form gathers details for each individual. Both forms aim to ensure that the correct patient receives the appropriate benefits and that all necessary information is captured for processing claims.
Lastly, the Durable Medical Equipment (DME) Claim Form bears resemblance to the Express Scripts Fax form. Both forms are used to request reimbursement for specific medical supplies and equipment. The DME Claim Form requires information about the patient, the equipment being claimed, and details about the prescribing physician. Similar to the Express Scripts form, it also necessitates the submission of receipts or documentation to support the claim. This ensures that the claims are processed accurately and efficiently, reflecting the same level of detail and verification required in both documents.
When filling out the Express Scripts Fax form, there are several important dos and don'ts to keep in mind to ensure a smooth submission process. Here’s a helpful list:
By following these guidelines, you can help ensure that your claim is processed efficiently and without unnecessary complications.
Misunderstandings about the Express Scripts Fax form can lead to confusion and delays in processing claims. Here are nine common misconceptions, along with clarifications for each.
Understanding these misconceptions can help ensure a smoother experience when submitting claims through the Express Scripts Fax form.
Filling out the Express Scripts Fax form correctly is essential for ensuring timely processing of prescription drug claims. Here are five key takeaways:
Following these guidelines will help streamline the claims process and minimize the risk of issues arising during submission.