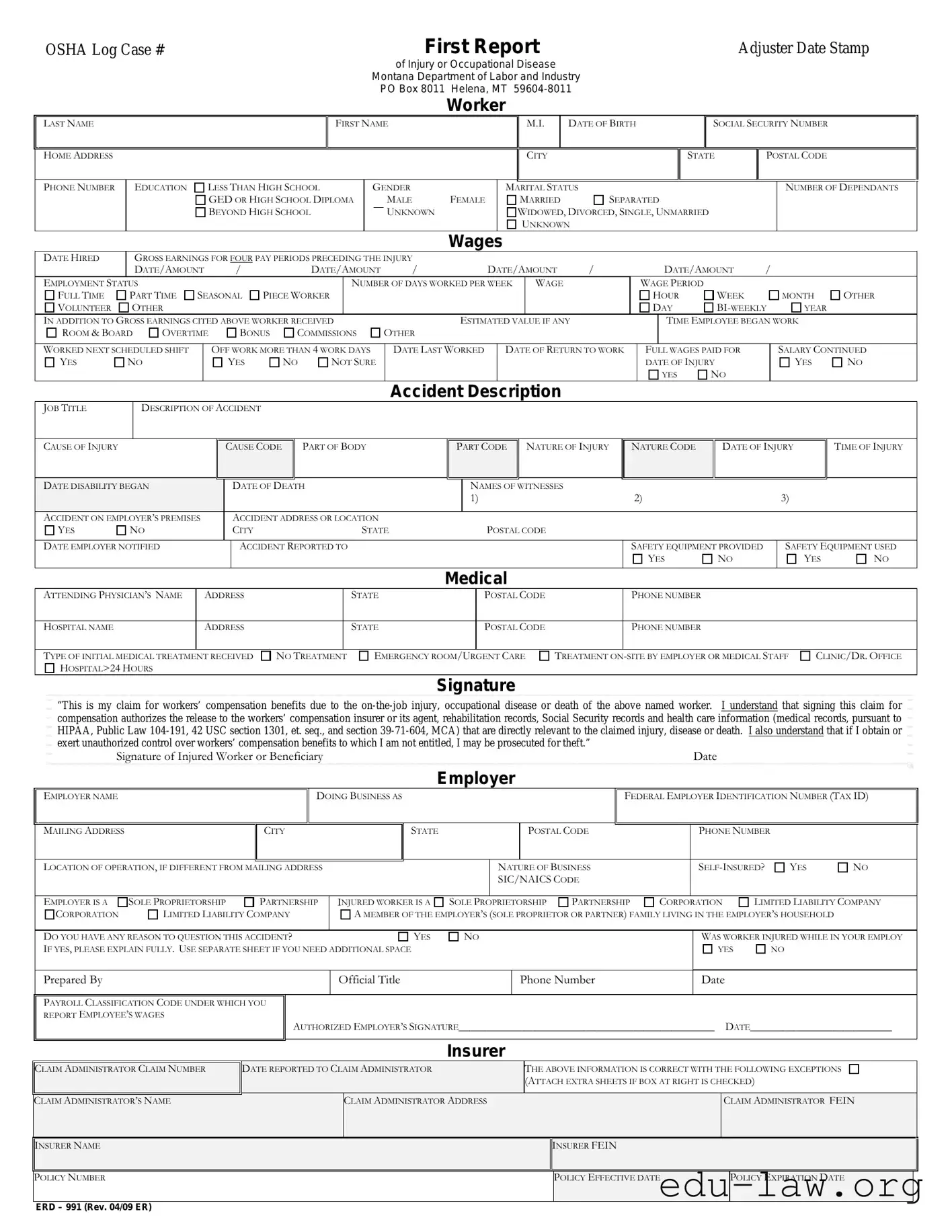
The ERD 991 form is a crucial document utilized in the workers' compensation process, specifically designed for reporting on-the-job injuries, occupational diseases, or fatalities. This form is mandated by the Montana Department of Labor and Industry and serves multiple purposes, including capturing essential details about the injured worker and the circumstances surrounding the incident. Key sections of the form require information such as the worker's personal details, including their name, address, date of birth, and Social Security number. It also prompts the reporting of the injury's specifics, including the date, time, and nature of the incident, as well as the medical treatment received. Employers are tasked with providing their information, including business structure and insurance details, ensuring a comprehensive overview of the situation. Additionally, the form includes a section for signatures, affirming the accuracy of the information provided and the worker's understanding of their rights and responsibilities regarding workers' compensation benefits. Completing the ERD 991 form accurately and promptly is vital for ensuring that injured workers receive the benefits they are entitled to, thus facilitating a smoother recovery process and minimizing potential disputes.
OSHA Log Case #
First Report |
Adjuster Date Stamp |
of Injury or Occupational Disease
Montana Department of Labor and Industry PO Box 8011 Helena, MT
Worker
LAST NAME
HOME ADDRESS
FIRST NAME
M.I. |
DATE OF BIRTH |
|
|
CITY |
|
|
|
SOCIAL SECURITY NUMBER
STATE |
POSTAL CODE |
|
|
PHONE NUMBER
EDUCATION
LESS THAN HIGH SCHOOL
GED OR HIGH SCHOOL DIPLOMA
BEYOND HIGH SCHOOL
GENDER
MALE
UNKNOWN
FEMALE
MARITAL STATUS
MARRIED SEPARATED
WIDOWED, DIVORCED, SINGLE, UNMARRIED
UNKNOWN
NUMBER OF DEPENDANTS
Wages
|
DATE HIRED |
|
GROSS EARNINGS FOR FOUR PAY PERIODS PRECEDING THE INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
|
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|||||||||||||
|
EMPLOYMENT STATUS |
|
|
|
|
|
|
|
|
|
|
|
NUMBER OF DAYS WORKED PER WEEK |
WAGE |
|
|
|
WAGE PERIOD |
|
|
|
|
|
|
|||||||||||
|
FULL TIME |
PART TIME |
SEASONAL |
PIECE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
HOUR |
|
WEEK |
|
|
MONTH |
OTHER |
|||||||||||
|
VOLUNTEER |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAY |
|
YEAR |
|
||||||
|
IN ADDITION TO GROSS EARNINGS CITED ABOVE WORKER RECEIVED |
|
|
|
|
ESTIMATED VALUE IF ANY |
|
|
|
|
TIME EMPLOYEE BEGAN WORK |
|
|||||||||||||||||||||||
|
ROOM & BOARD |
OVERTIME |
|
|
|
BONUS |
|
COMMISSIONS |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
WORKED NEXT SCHEDULED SHIFT |
|
|
OFF WORK MORE THAN 4 WORK DAYS |
|
DATE LAST WORKED |
|
DATE OF RETURN TO WORK |
|
FULL WAGES PAID FOR |
|
|
SALARY CONTINUED |
||||||||||||||||||||||
|
YES |
NO |
|
|
|
|
|
YES |
|
NO |
NOT SURE |
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF INJURY |
|
|
YES |
NO |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Description |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
JOB TITLE |
|
DESCRIPTION OF ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
CAUSE OF INJURY |
|
|
|
|
|
|
|
CAUSE CODE |
|
|
PART OF BODY |
|
|
|
PART CODE |
NATURE OF INJURY |
|
NATURE CODE |
|
DATE OF INJURY |
TIME OF INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
DATE OF DEATH |
|
|
|
|
NAMES OF WITNESSES |
|
|
2) |
|
|
|
|
|
3) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
ACCIDENT ON EMPLOYER’S PREMISES |
|
|
|
ACCIDENT ADDRESS OR LOCATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
YES |
NO |
|
|
|
|
|
|
CITY |
|
|
|
|
STATE |
|
|
|
|
POSTAL CODE |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
DATE EMPLOYER NOTIFIED |
|
|
|
|
|
|
ACCIDENT REPORTED TO |
|
|
|
|
|
|
|
|
|
|
|
SAFETY EQUIPMENT PROVIDED |
|
|
SAFETY EQUIPMENT USED |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical
ATTENDING PHYSICIAN’S NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
PHONE NUMBER |
|
|
|
|
|
|
PHONE NUMBER |
HOSPITAL NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
|
|
|
|
|
|
|
|
TYPE OF INITIAL MEDICAL TREATMENT |
RECEIVED |
NO TREATMENT |
EMERGENCY ROOM/U |
RGENT CARE |
TREATMENT ON |
|
HOSPITAL>24 HOURS |
|
|
|
|
|
|
CLINIC/DR. OFFICE
Signature
“This is my claim for workers’ compensation benefits due to the
Signature of Injured Worker or Beneficiary |
Date |
Employer
EMPLOYER NAME
DOING BUSINESS AS
FEDERAL EMPLOYER IDENTIFICATION NUMBER (TAX ID)
MAILING ADDRESS |
|
CITY |
|
STATE |
|
|
|
POSTAL CODE |
|
PHONE NUMBER |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
LOCATION OF OPERATION, IF DIFFERENT FROM MAILING ADDRESS |
|
|
|
NATURE OF BUSINESS |
|
YES |
NO |
||||||||
|
|
|
|
|
|
|
SIC/NAICS CODE |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIMITED LIABILITY COMPANY |
||||
EMPLOYER IS A |
SOLE PROPRIETORSHIP |
PARTNERSHIP |
INJURED WORKER IS A |
SOLE P |
ROPRIETORSHIP |
PARTNERSHIP |
CORPORATION |
||||||||
CORPORATION |
LIMITED LIABILITY COMPANY |
A MEMBER OF THE EMPLOYER’S (SOLE PROPRIETOR OR PARTNER) FAMILY LIVING IN THE EMPLOYER’S HOUSEHOLD |
|
||||||||||||
|
|
|
|
|
|
|
|
WAS WORKER INJURED WHILE IN YOUR EMPLOY |
|||||||
DO YOU HAVE ANY REASON TO QUESTION THIS ACCIDENT? |
|
YES |
NO |
|
|
||||||||||
IF YES, PLEASE EXPLAIN FULLY. USE SEPARATE SHEET IF YOU NEED ADDITIONAL SPACE |
|
|
|
|
|
|
YES |
NO |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Prepared By |
|
|
|
Official Title |
|
|
|
Phone Number |
|
Date |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PAYROLL CLASSIFICATION CODE UNDER WHICH YOU |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
REPORT EMPLOYEE’S WAGES |
|
AUTHORIZED EMPLOYER’S SIGNATURE_______________________________________________ |
DATE__________________________ |
||||||||||||
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurer
CLAIM ADMINISTRATOR CLAIM NUMBER
DATE REPORTED TO CLAIM ADMINISTRATOR
THE ABOVE INFORMATION IS CORRECT WITH THE FOLLOWING EXCEPTIONS (ATTACH EXTRA SHEETS IF BOX AT RIGHT IS CHECKED)
CLAIM ADMINISTRATOR’S NAME |
CLAIM ADMINISTRATOR ADDRESS |
|
CLAIM ADMINISTRATOR FEIN |
|
|
|
|
|
|
|
|
INSURER NAME |
|
INSURER FEIN |
|
|
|
|
|
|
|
|
|
POLICY NUMBER |
|
POLICY EFFECTIVE DATE |
|
POLICY EXPIRATION DATE |
|
|
|
|
|
|
|
ERD – 991 (Rev. 04/09 ER)
| Fact Name | Details |
|---|---|
| Form Purpose | The ERD 991 form is used to file a claim for workers' compensation benefits in Montana. |
| Governing Law | This form is governed by Montana Code Annotated (MCA) Title 39, Chapter 71. |
| Department | The form is administered by the Montana Department of Labor and Industry. |
| Injury Reporting | It requires details about the date and nature of the injury or occupational disease. |
| Employee Information | Workers must provide personal details, including name, address, and social security number. |
| Employer Information | Employers must include their name, address, and federal employer identification number. |
| Medical Treatment | Information about initial medical treatment received must be documented on the form. |
| Witnesses | The form allows for the inclusion of witness names related to the accident. |
| Signature Requirement | The injured worker or beneficiary must sign the form to authorize the claim. |
Completing the ERD 991 form requires careful attention to detail and accuracy. This form is essential for reporting workplace injuries or occupational diseases and must be filled out completely to ensure proper processing. Below are the steps to guide you through the process of filling out the form correctly.
After completing the form, review it for accuracy before submission. Ensure that all required fields are filled out and that the information provided is correct. This careful preparation will facilitate the processing of the claim and help avoid potential delays.
What is the ERD 991 form used for?
The ERD 991 form is a crucial document for reporting workplace injuries or occupational diseases in Montana. It serves as the First Report of Injury and is submitted to the Montana Department of Labor and Industry. This form helps initiate the workers' compensation process, ensuring that injured workers receive the benefits they are entitled to after an incident occurs on the job.
Who is responsible for filling out the ERD 991 form?
The injured worker or their beneficiary typically fills out the ERD 991 form. However, employers also play a role in the process. They must provide certain information about the incident, including details about the worker's employment status and the nature of the accident. Both parties need to ensure that the form is completed accurately to avoid delays in the claims process.
What information is required on the ERD 991 form?
The ERD 991 form requires various pieces of information. Key details include the worker's name, address, date of birth, social security number, and employment details. It also asks for specifics about the injury, such as the date, time, and description of the accident, as well as any medical treatment received. Accurate and complete information is vital to facilitate the processing of the claim.
What happens after the ERD 991 form is submitted?
Once the ERD 991 form is submitted, it is reviewed by the claims administrator. They will assess the information provided and determine the eligibility of the worker for benefits. This process may involve communication with the employer, the injured worker, and medical providers. If approved, the injured worker will receive compensation for medical expenses and lost wages related to the injury.
Can the ERD 991 form be amended after submission?
Yes, the ERD 991 form can be amended after submission if there are any errors or additional information that needs to be included. It is important to communicate these changes to the claims administrator promptly. Keeping the information accurate ensures that the claim is processed correctly and that the injured worker receives the appropriate benefits.
Is there a deadline for submitting the ERD 991 form?
Yes, there is a deadline for submitting the ERD 991 form. Generally, it should be filed as soon as possible after the injury occurs, typically within 30 days. Timely submission is essential to avoid complications with the claim and to ensure that the injured worker can access benefits without unnecessary delays.
Incomplete Information: Failing to fill out all required fields can lead to delays. Ensure that every section is completed, including names, addresses, and social security numbers.
Incorrect Dates: Entering the wrong date of injury or the date of last work can cause confusion. Double-check these dates for accuracy.
Improper Signature: The form must be signed by the injured worker or beneficiary. An unsigned form will not be processed.
Missing Medical Information: Not providing the attending physician’s details can hinder the claim process. Include the physician's name, address, and contact information.
Neglecting to Report Witnesses: If there were witnesses to the accident, failing to include their names and contact information can weaken the claim.
Inaccurate Employment Status: Misrepresenting the employment status, such as full-time or part-time, can lead to complications in processing the claim.
Not Providing Additional Documentation: If there are exceptions or additional information, not attaching extra sheets can result in incomplete claims. Always provide supporting documents when necessary.
The ERD 991 form is essential for filing a workers' compensation claim in Montana. It gathers crucial information about the injured worker, the incident, and the employer. Alongside this form, several other documents may be necessary to ensure a complete and accurate claim process. Below is a list of commonly used forms and documents that accompany the ERD 991 form.
Each of these documents plays a vital role in the workers' compensation process, ensuring that all necessary information is available for the claim to be evaluated thoroughly. Having these forms ready can help streamline the process and support the injured worker in receiving the benefits they deserve.
The ERD 991 form is similar to the OSHA 300 Log, which is used to record workplace injuries and illnesses. Both documents serve the purpose of documenting incidents that occur in the workplace, focusing on the details of the injury or illness. The OSHA 300 Log requires employers to record the date of the incident, the nature of the injury, and the affected body part, much like the ERD 991. Both forms are essential for compliance with workplace safety regulations and help track injury trends over time.
Another document that parallels the ERD 991 is the First Report of Injury (FROI) form. This form is often the initial notification of an injury to an insurance company or state agency. Similar to the ERD 991, the FROI collects information about the injured worker, including their personal details, the circumstances of the injury, and the medical treatment received. Both forms are crucial for initiating the workers' compensation claim process and ensuring that all necessary information is provided promptly.
The Workers' Compensation Claim Form is another document akin to the ERD 991. This form is used to formally file a claim for workers' compensation benefits. Like the ERD 991, it requires detailed information about the injured worker, the injury, and the employer. Both forms aim to facilitate the claims process, ensuring that all relevant information is collected to support the worker's claim for benefits.
Similar to the ERD 991 is the Medical Report of Injury form. This document provides detailed medical information regarding the injury, including diagnoses, treatment plans, and the worker’s recovery status. Both forms require the involvement of medical professionals and are essential for establishing the extent of the injury and the necessary medical care, thus aiding in the compensation process.
The Employer's Incident Report also shares similarities with the ERD 991. This internal document is used by employers to record the specifics of an incident that occurs at the workplace. It captures details such as the time, place, and nature of the incident, much like the ERD 991. Both forms help employers analyze incidents for safety improvements and compliance with reporting requirements.
The Employee Injury Report form is another document that is comparable to the ERD 991. This form is typically filled out by the injured worker and includes personal information, details of the injury, and circumstances surrounding the incident. Both forms emphasize the importance of accurate reporting and documentation to ensure that claims are processed efficiently and fairly.
Lastly, the Return to Work form is similar to the ERD 991 in that it documents the worker's status after an injury. This form outlines the worker’s ability to return to their job, any restrictions, and the date of return. Both documents are critical in managing the workers' compensation process, ensuring that all parties are informed about the worker's recovery and readiness to resume their duties.
When filling out the ERD 991 form, it’s important to ensure accuracy and completeness. Here are some things you should and shouldn't do:
Misunderstandings about the ERD 991 form can lead to confusion and complications in the workers' compensation process. Here are ten common misconceptions, clarified for better understanding:
Understanding these misconceptions can help ensure that injured workers navigate the claims process more effectively. Accurate information is key to securing the benefits they deserve.
When filling out the ERD 991 form, it’s essential to ensure accuracy and completeness. Here are some key takeaways to keep in mind:
By following these key points, you can help ensure that the ERD 991 form is filled out correctly, paving the way for a smoother claims process.