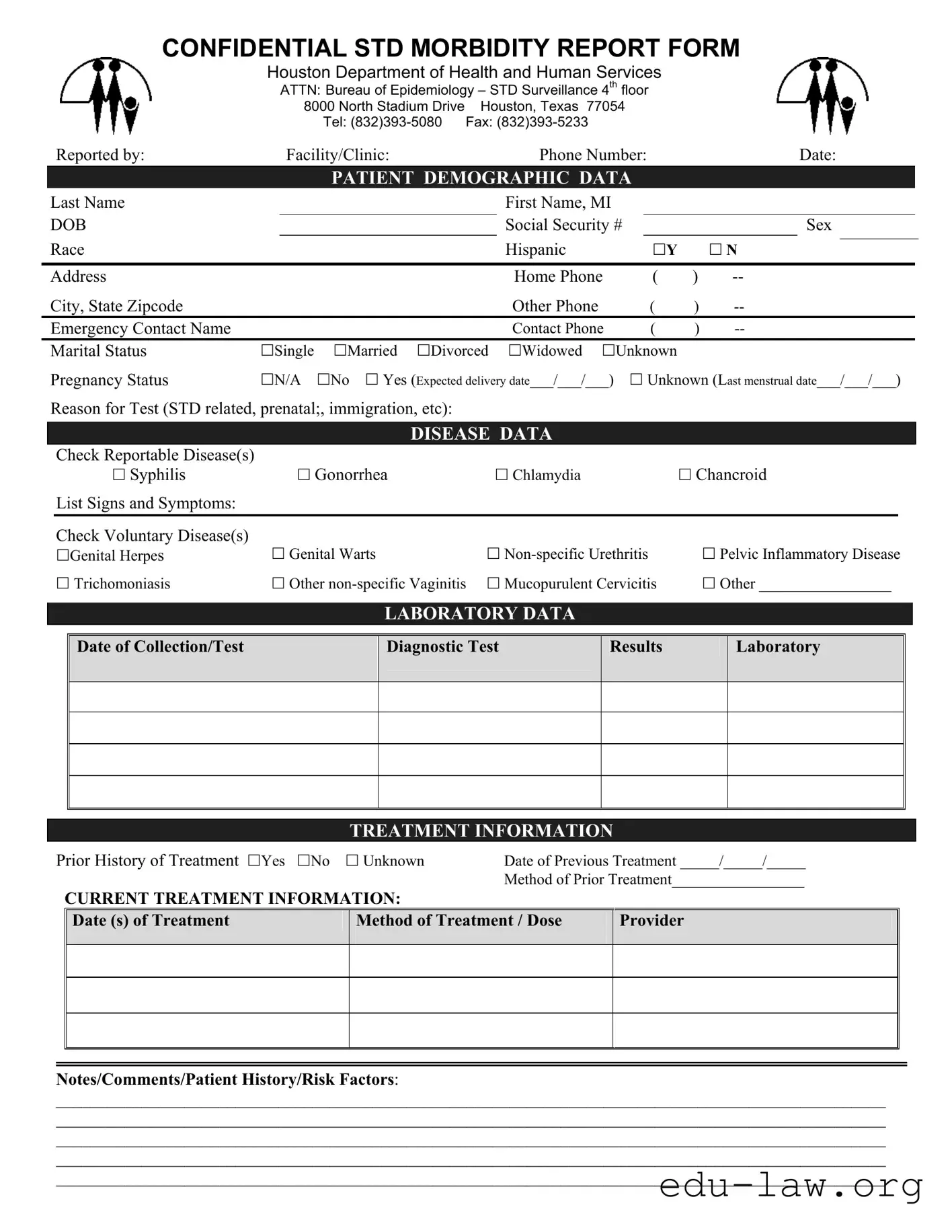
The Connecticut UC 2 form plays a crucial role in public health, particularly in the surveillance and reporting of sexually transmitted diseases (STDs). Designed for use by healthcare facilities and clinics, this form collects essential demographic information about patients, including their names, contact details, and medical history. It also requires the reporting of specific diseases, such as syphilis, gonorrhea, and chlamydia, along with any associated signs and symptoms. Healthcare providers must document laboratory data, including test dates and results, to ensure accurate tracking of disease prevalence. Treatment information is another vital component, as it captures prior and current treatment details, allowing for a comprehensive understanding of each patient's medical journey. Additionally, the form includes sections for notes and comments, enabling providers to share relevant patient history and risk factors. By facilitating thorough and confidential reporting, the Connecticut UC 2 form helps public health officials monitor and respond to STD trends effectively, ultimately contributing to better health outcomes for the community.
CONFIDENTIAL STD MORBIDITY REPORT FORM
Houston Department of Health and Human Services
ATTN: Bureau of Epidemiology – STD Surveillance 4th floor
8000 North Stadium Drive Houston, Texas 77054
Tel:
|
|
Reported by: |
|
Facility/Clinic: |
|
Phone Number: |
|
|
Date: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
PATIENT DEMOGRAPHIC DATA |
|
|
|
|
|
|
|||||
|
Last Name |
|
|
|
|
|
First Name, MI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOB |
|
|
|
|
|
Social Security # |
|
|
|
Sex |
|
||||
|
Race |
|
|
|
|
|
Hispanic |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Y |
|
N |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Home Phone |
( |
) |
|
|
|
|
|||
|
City, State Zipcode |
|
|
|
|
|
Other Phone |
( |
) |
|
|
|
|
|||
|
Emergency Contact Name |
|
|
|
|
|
Contact Phone |
( |
) |
|
|
|
|
|||
|
Marital Status |
Single |
Married |
Divorced |
Widowed |
Unknown |
|
|
|
|
|
|
||||
|
Pregnancy Status |
N/A |
No |
Yes (Expected delivery date___/___/___) |
|
Unknown (Last menstrual date___/___/___) |
|
|||||||||
|
Reason for Test (STD related, prenatal;, immigration, etc): |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISEASE DATA |
|
|
|
|
|
|
|
|
|
|
|
Check Reportable Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Syphilis |
|
|
Gonorrhea |
|
Chlamydia |
|
|
Chancroid |
|
|||||
|
|
List Signs and Symptoms: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check Voluntary Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Genital Herpes |
|
Genital Warts |
|
|
|
Pelvic Inflammatory Disease |
|
|||||||
|
|
Trichomoniasis |
|
Other |
Mucopurulent Cervicitis |
|
Other _________________ |
|
||||||||
LABORATORY DATA
Date of Collection/Test
Diagnostic Test
Results
Laboratory
TREATMENT INFORMATION
Prior History of Treatment Yes No |
Unknown |
Date of Previous Treatment _____/_____/_____ |
|
||
|
|
|
Method of Prior Treatment_________________ |
|
|
|
CURRENT TREATMENT INFORMATION: |
|
|
|
|
|
Date (s) of Treatment |
Method of Treatment / Dose |
Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes/Comments/Patient History/Risk Factors:
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
| Fact Name | Description |
|---|---|
| Form Purpose | The Connecticut UC 2 form is used for reporting confidential STD morbidity data. |
| Governing Law | This form is governed by Connecticut General Statutes, Section 19a-216. |
| Submitting Authority | The form must be submitted to the Bureau of Epidemiology – STD Surveillance. |
| Contact Information | For inquiries, contact the Houston Department of Health and Human Services at (832) 393-5080. |
| Patient Demographics | Essential patient information includes name, date of birth, and contact details. |
| Reportable Diseases | The form allows for the reporting of diseases like Syphilis, Gonorrhea, and Chlamydia. |
| Voluntary Diseases | Conditions such as Genital Herpes and Pelvic Inflammatory Disease can also be reported. |
| Treatment History | Providers must indicate any prior treatment history for the patient. |
| Confidentiality | The form ensures that all reported information remains confidential. |
| Submission Deadline | Timely submission is crucial for effective disease surveillance and response. |
Filling out the Connecticut UC 2 form requires careful attention to detail to ensure that all necessary information is accurately reported. Once completed, the form will be submitted to the appropriate health department for processing. Follow these steps to fill out the form correctly.
What is the purpose of the Connecticut UC 2 form?
The Connecticut UC 2 form serves as a confidential morbidity report for sexually transmitted diseases (STDs). It is utilized by healthcare providers to report cases of specific reportable diseases, such as syphilis, gonorrhea, and chlamydia, to the appropriate health authorities. This data is essential for public health monitoring and intervention strategies aimed at controlling the spread of STDs.
Who is responsible for filling out the UC 2 form?
Healthcare professionals at clinics and facilities that diagnose or treat STDs are responsible for completing the UC 2 form. This includes physicians, nurses, and other medical staff who have access to patient information. Accurate completion of the form is crucial for effective disease surveillance and management.
What information is required on the UC 2 form?
The UC 2 form requires detailed patient demographic data, including the patient's name, date of birth, social security number, and contact information. Additionally, it collects information about the reported disease, laboratory test results, treatment history, and current treatment details. This comprehensive data helps health authorities understand and respond to STD trends effectively.
How is patient confidentiality maintained when using the UC 2 form?
Confidentiality is a top priority when handling the UC 2 form. The form is designed to protect sensitive patient information, and only authorized personnel have access to the completed reports. Facilities must ensure that all data is stored securely and shared only with relevant public health agencies, adhering to privacy regulations.
What should be done if a healthcare provider has questions about filling out the UC 2 form?
If a healthcare provider has questions regarding the completion of the UC 2 form, they should reach out to the Houston Department of Health and Human Services, specifically the Bureau of Epidemiology – STD Surveillance. The contact number is (832) 393-5080, where assistance can be provided to clarify any uncertainties related to the form's requirements.
What happens to the information submitted on the UC 2 form?
Once submitted, the information on the UC 2 form is analyzed by public health officials to track disease trends, identify outbreaks, and implement prevention strategies. The data plays a critical role in public health initiatives, allowing for targeted education and treatment efforts aimed at reducing the incidence of STDs in the community.
Failing to provide complete patient demographic data. Missing information such as the last name, first name, or date of birth can lead to processing delays.
Not including the correct social security number. An incorrect or missing social security number can complicate identification and reporting.
Leaving out the reason for the test. This information is crucial for understanding the context of the diagnosis.
Checking incorrect disease categories. Ensure that the reportable and voluntary diseases checked accurately reflect the patient's condition.
Not documenting laboratory data properly. Include the date of collection and test results to avoid confusion.
Overlooking the treatment information. It is important to accurately report any prior treatments and current treatment details.
Failing to provide emergency contact information. This can hinder communication in urgent situations.
Not specifying marital status or pregnancy status correctly. This information can be relevant for certain health assessments.
Neglecting to add notes or comments about patient history or risk factors. This information can be vital for future care.
Submitting the form without a signature or date. Ensure that the form is signed and dated to validate the information provided.
The Connecticut UC-2 form is a vital document used for reporting morbidity related to sexually transmitted diseases (STDs). It ensures that health authorities can track and manage public health concerns effectively. Along with the UC-2 form, several other forms and documents are often utilized to support the reporting process and ensure comprehensive patient care. Below is a list of these related documents.
These documents work together to ensure that health care providers can deliver comprehensive and effective care for patients dealing with STDs. By utilizing these forms, healthcare professionals can enhance communication, improve patient outcomes, and contribute to public health efforts.
The Connecticut UC-2 form is similar to the CDC's STD Surveillance Report. Both documents serve the purpose of collecting detailed information about sexually transmitted diseases. The STD Surveillance Report requires demographic data, clinical findings, and laboratory results, just like the UC-2 form. This consistency ensures that health departments can monitor and respond to STD outbreaks effectively. Both forms emphasize the importance of accurate reporting for public health initiatives, allowing for better tracking of disease trends and resource allocation.
Another document that aligns closely with the Connecticut UC-2 form is the Patient Health History Form used in many medical facilities. This form gathers comprehensive patient information, including demographics, medical history, and current symptoms. Similar to the UC-2, it aims to create a complete picture of a patient's health status. The inclusion of treatment history and current medications in both forms highlights the necessity of understanding a patient's background for effective care and management.
The National Notifiable Diseases Surveillance System (NNDSS) form is also comparable to the Connecticut UC-2 form. NNDSS collects data on various communicable diseases, including STDs. Both forms require healthcare providers to report specific diseases and symptoms, ensuring that public health officials receive timely information. This data is crucial for identifying trends and implementing prevention strategies, making both forms vital tools in public health surveillance.
Additionally, the Infectious Disease Report Form used by many state health departments shares similarities with the UC-2 form. This report also collects patient demographics, disease specifics, and treatment information. The structure and purpose of both forms facilitate the efficient gathering of essential health data, enabling state agencies to monitor infectious disease outbreaks and respond appropriately to public health threats.
The Medical History Questionnaire, often used in clinical settings, can be compared to the Connecticut UC-2 form as well. This questionnaire captures patient demographics, previous medical treatments, and current health concerns. Like the UC-2, it aims to provide healthcare providers with the information necessary to deliver effective care. Both documents underscore the importance of understanding a patient’s medical background to inform treatment decisions.
Lastly, the Health Insurance Portability and Accountability Act (HIPAA) Compliance Form is relevant in this context. While its primary purpose is to ensure patient privacy, it often requires similar demographic and treatment information as the UC-2 form. Both documents prioritize patient confidentiality while collecting essential health data, ensuring that providers can deliver appropriate care while adhering to legal requirements regarding privacy and security.
When filling out the Connecticut UC 2 form, it is essential to follow certain guidelines to ensure accuracy and compliance. Below is a list of dos and don’ts to consider.
Misconception 1: The Connecticut UC 2 form is only for reporting STD cases.
In reality, the form can also be used for other health-related reporting, such as prenatal or immigration-related tests.
Misconception 2: The information on the UC 2 form is not confidential.
Actually, the form is designed to protect patient confidentiality. Sensitive information is handled with care to maintain privacy.
Misconception 3: Only doctors can fill out the UC 2 form.
Healthcare providers, including nurses and clinic staff, can complete the form. They are trained to gather the necessary information.
Misconception 4: The UC 2 form must be submitted immediately after a test.
While timely reporting is important, there may be specific deadlines set by the health department for submission.
Misconception 5: Patients need to provide their Social Security number on the UC 2 form.
Providing a Social Security number is optional. Patients can choose not to disclose this information if they prefer.
Misconception 6: The UC 2 form only tracks positive test results.
The form can also include negative test results, as it helps in understanding the overall health trends in the community.
When filling out and using the Connecticut UC 2 form, there are several important points to keep in mind. This form is essential for reporting certain health-related information, particularly regarding sexually transmitted diseases (STDs). Here are some key takeaways: