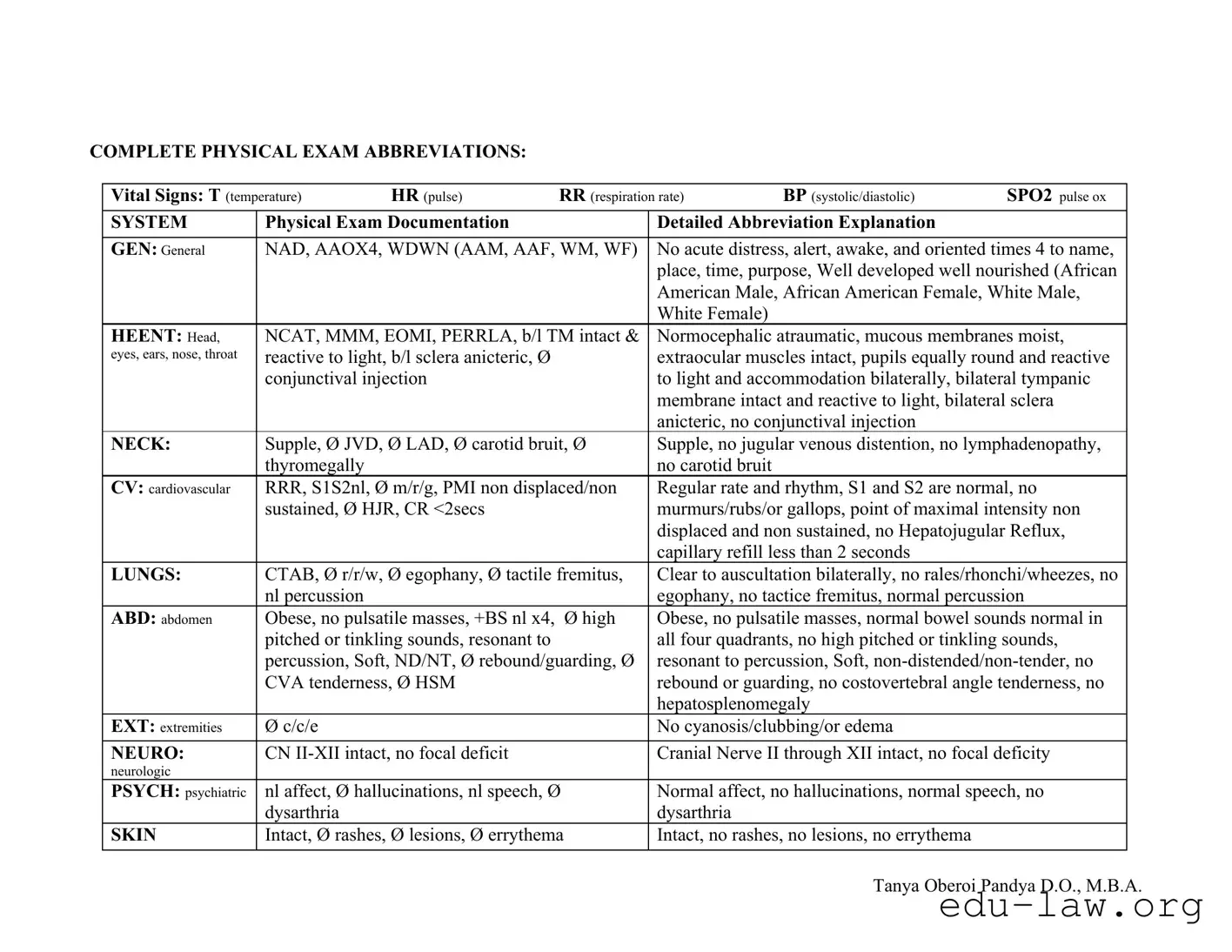
The Complete Physical Examination form is a vital tool used by healthcare providers to document a comprehensive assessment of a patient's health status. This form encompasses a variety of critical components, including vital signs such as temperature, heart rate, respiration rate, blood pressure, and oxygen saturation levels. It also details the physical examination findings across multiple body systems, including general appearance, head, eyes, ears, nose, and throat (HEENT), cardiovascular, respiratory, abdominal, neurological, and musculoskeletal evaluations. Each section employs standardized abbreviations and terminology to ensure clarity and consistency in reporting. For instance, findings may indicate whether a patient is in acute distress, the presence or absence of murmurs in the cardiovascular assessment, or the condition of the abdomen. Additionally, the form addresses genitourinary, psychiatric, and skin assessments, providing a holistic view of the patient's health. By utilizing this form, healthcare professionals can efficiently communicate essential information, aiding in diagnosis, treatment planning, and ongoing patient care.
COMPLETE PHYSICAL EXAM ABBREVIATIONS:
Vital Signs: T (temperature) |
HR (pulse) |
RR (respiration rate) |
BP (systolic/diastolic) |
SPO2 pulse ox |
||
|
|
|
|
|
||
SYSTEM |
Physical Exam Documentation |
|
Detailed Abbreviation Explanation |
|
||
|
|
|
||||
GEN: General |
NAD, AAOX4, WDWN (AAM, AAF, WM, WF) |
No acute distress, alert, awake, and oriented times 4 to name, |
||||
|
|
|
|
place, time, purpose, Well developed well nourished (African |
||
|
|
|
|
American Male, African American Female, White Male, |
||
|
|
|
|
White Female) |
|
|
HEENT: Head, |
NCAT, MMM, EOMI, PERRLA, b/l TM intact & |
Normocephalic atraumatic, mucous membranes moist, |
||||
eyes, ears, nose, throat |
reactive to light, b/l sclera anicteric, Ø |
|
extraocular muscles intact, pupils equally round and reactive |
|||
|
conjunctival injection |
|
to light and accommodation bilaterally, bilateral tympanic |
|||
|
|
|
|
membrane intact and reactive to light, bilateral sclera |
||
|
|
|
|
anicteric, no conjunctival injection |
|
|
NECK: |
Supple, Ø JVD, Ø LAD, Ø carotid bruit, Ø |
Supple, no jugular venous distention, no lymphadenopathy, |
||||
|
thyromegally |
|
|
no carotid bruit |
|
|
CV: cardiovascular |
RRR, S1S2nl, Ø m/r/g, PMI non displaced/non |
Regular rate and rhythm, S1 and S2 are normal, no |
||||
|
sustained, Ø HJR, CR <2secs |
|
murmurs/rubs/or gallops, point of maximal intensity non |
|||
|
|
|
|
displaced and non sustained, no Hepatojugular Reflux, |
||
|
|
|
|
capillary refill less than 2 seconds |
|
|
LUNGS: |
CTAB, Ø r/r/w, Ø egophany, Ø tactile fremitus, |
Clear to auscultation bilaterally, no rales/rhonchi/wheezes, no |
||||
|
nl percussion |
|
|
egophany, no tactice fremitus, normal percussion |
||
ABD: abdomen |
Obese, no pulsatile masses, +BS nl x4, |
Ø high |
Obese, no pulsatile masses, normal bowel sounds normal in |
|||
|
pitched or tinkling sounds, resonant to |
|
all four quadrants, no high pitched or tinkling sounds, |
|||
|
percussion, Soft, ND/NT, Ø rebound/guarding, Ø |
resonant to percussion, Soft, |
||||
|
CVA tenderness, Ø HSM |
|
rebound or guarding, no costovertebral angle tenderness, no |
|||
|
|
|
|
hepatosplenomegaly |
|
|
EXT: extremities |
Ø c/c/e |
|
|
No cyanosis/clubbing/or edema |
|
|
|
|
|
|
|||
NEURO: |
CN |
|
Cranial Nerve II through XII intact, no focal deficity |
|||
neurologic |
|
|
|
|
|
|
PSYCH: psychiatric |
nl affect, Ø hallucinations, nl speech, Ø |
Normal affect, no hallucinations, normal speech, no |
||||
|
dysarthria |
|
|
dysarthria |
|
|
SKIN |
Intact, Ø rashes, Ø lesions, Ø errythema |
Intact, no rashes, no lesions, no errythema |
|
|||
|
|
|
|
|
|
|
Tanya Oberoi Pandya D.O., M.B.A.

GU: (genitourinary) |
Male: Ø rashes, Ø penile discharge, penile shaft s |
Male: no rashes, no penile discharge, penile shaft without |
|
masses or lesions, Ø inguinal hernia, Ø inguinal |
masses or lesions, no inguinal hernia, no inguinal |
|
LAD, b/l testicles nl in consistency s hydrocele or |
lymphadenopathy, bilateral testicles normal in consistency |
|
varicocele, Ø hypospadias/epispadias |
without hydrocele or varicocele, no hypospadias or |
|
|
epispadias |
Pelvic: |
Ø rashes, nl bartholin gland, vaginal mucosa nl |
No rashes, normal bartholin gland, vaginal mucosa of normal |
|
consistency s atrophy or discharge, cervical os s |
consistency without atrophy or discharge, cervical os without |
|
discharge |
discharge |
|
Bimanual: Ø CMT Ø VB Ø discharge Ømasses |
Bimanual: No cervical motion tenderness, no vaginal |
|
|
bleeding, no discharge, no masses |
RECTAL |
Ø BRBPR, Ø melena, Ø masses, nl sphincter |
No bright red blood per rectum, no melena, no masses, |
|
tone, Ø ext/int hemorrhoids, prostate walnut size |
normal sphincter tone, no external or internal hemorrhoids, |
|
s nodularity or hypertrophy, Ø prostate tenderness |
prostate walnut size without nodularity or hypertrophy, no |
|
|
prostate tenderness |
LYMPH: |
Ø LAD |
No lymphadenopathy |
(lymphatic) |
|
|
Mmsk: |
nl ROM, Ø joint swelling or errythema |
Normal range of motion, no joint swelling or errythema |
(musculoskeletal) |
|
|
Tanya Oberoi Pandya D.O., M.B.A.
COMMON ABREVIATIONS ENCOUNTERED IN PRACTICE:
CC |
Chief complaint |
HPI |
History of Present Illness |
ROS |
Review of System |
PMH |
Past Medical History |
NKDA |
No known Drug Allergies |
CP |
Chest Pain |
|
|
SOB |
Shortness of Breath |
DOE |
Dyspnea on exertion |
PND |
If talking cardiac: Paroxysmal Nocturnal Dyspnea |
|
If talking Upper respiratory: Post Nasal Drip |
JVD |
Jugular Venous Distention |
HJR |
|
LE edema |
Lower Extremity edema |
No c/c/e |
No cyanosis/clubbing/edema |
No r/r/w |
No Rales/rhonchi/wheezes |
No m/r/g |
No murmurs/rubs/gallops |
CTAB |
Clear To Auscultation Bilaterally |
RRR |
Regular Rate and Rhythm |
S1S2 nl |
S1 (first heart sound) and S2 (second heart sound) |
|
are normal in auscultation |
EKG: |
|
LAD |
Left Axis Deviation |
RAD |
Right Axis Deviation |
RAE |
Right Atrial Enlargement |
LAE |
Left Atrial Enlargement |
LVH |
Left Ventricular Hypertrophy |
NSR |
Normal Sinus Rhythm |
LAD |
Lymphadenopathy |
EOMI |
|
PERRL |
Pupils Equally Round and Reactive to light |
Cranial Nerves two through twelve intact |
|
MMSE |
Mini Mental Status Exam |
No T/A/D |
No Tobacco/Alcohol/IV drug use |
Ctx |
Contractions |
Fx |
Fracture or function (depending on context) |
P.V. |
Per Vagina |
P.R. |
Per Rectum |
SBP |
Systolic Blood Pressure |
DBP |
Diastolic Blood Pressure |
HR |
Heart Rate |
RR |
Respiratory Rate |
SPO2 |
Pulse Oximetry |
BRBPR |
Bright Red Blood Per Rectum |
DTR |
Deep Tendon Reflexes |
ARF |
Acute Renal Failure |
CRI |
Chronic Renal Insufficiency |
CRF |
Chronic Renal Failure |
FEN/GI |
Fluids, Electrolytes, and |
|
Nutrition/Gastroenterology |
AAOX3 |
Alert, awake, and Oriented times 3 (to person, |
|
time, place) |
NAD |
No Acute Distress |
MMM |
Mucus Membranes Moist |
ND/NT |
Non Distended/Non Tender |
BSx4 |
Bowel Sounds present in all 4 quadrants |
N, V |
Nausea, Vomiting |
S.Q. |
Subcutaneous |
PTCA |
Percutaneous Transluminal Coronary Angioplasty |
PCI |
Percutaneous Intervention (cardiac) |
CAD |
Coronary Artery Disease |
ICD |
Implantable Cardioverter Defibrillator |
CABG |
Coronary Artery Bypass Graft |
VB |
Vaginal Bleeding |
FM |
Fetal Movement |
CMT |
Cervical motion tenderness |
LMP |
Last menstrual period |
NSVD |
Normal Spontaneous Vaginal Delivery |
PPROM |
Preterm Premature Rupture of Membranes |
PROM |
Premature Rupture of Membranes |
LTCS |
Low Transverse Cesarean Section |
VBAC |
Vaginal Birth After Cesarean Section |
EBL |
Estimated Blood Loss |
EGA |
Expected Gestational Age |
EDC |
Expected Date of Confinement (baby’s due date) |
Tanya Oberoi Pandya D.O., M.B.A.
IUP |
|
FHT |
Fetal Heart Tones |
TAH/BSO |
Total Abdominal Hysterectomy with Bilateral |
|
Salpigoopherectomy (i.e. no uterus/ tubes, no |
|
ovaries) |
TAH |
Total abdominal hysterectomy |
BTL |
Bilateral Tubal Ligation |
PTL |
Preterm Labor |
CVA |
Cerebrovascular accident |
TIA |
Transient Ischemic Attack |
No T/A/D |
No tobacco/alcohol/drugs |
Supp. |
Suppository |
Wt |
Weight |
HA |
Headache |
Palp |
Palpitations |
Sptm |
Sputum |
AGE |
Acute gastroenteritis |
URI |
Upper respiratory infection |
FH or FHx |
Family History |
SH or SHx |
Social history |
PVD |
Peripheral vascular disease |
DJD |
Degenerative joint disease |
OA |
Osteoarthritis |
POD |
Post Op Day |
Lap. chole. |
Laparoscopic Cholecystectomy |
Lap. Appy |
Laparoscopic appendectomy |
AKA |
Above the Knee Amputation |
BKA |
Below the Knee Amputation |
NKDA |
No Known Drug Allergies |
Hb |
Hemoglobin |
Hct |
Hematocrit |
H/H |
Hemoglobin and hematocrit |
CXR |
Chest |
BAL |
|
s/p |
Status post… |
h/o |
History of… |
wnl |
Within normal limits |
NC |
Non contributory (if written under family history) |
OA |
Osteoarthritis |
RCT |
Rotator cuff tear |
RTC |
Return to Clinic |
FOB |
Fecal Occult Blood |
AAAAbdominal Aortic Aneurysm
MURMURS:
AI |
Aortic Insufficiency |
AS |
Aortic Stenosis |
MR |
Mitral Regurgitation |
MS |
Mitral Stenosis |
TI |
Tricuspid Insufficiency |
PS |
Pulmonic Stenosis |
PI |
Pulmonic Insufficiency |
AVR |
Aortic Valve Replacement |
MVR |
Mitral Valve Replacement |
MVP |
Mitral Valve Prolapse |
AV |
Atrioventricular |
AVM |
|
UA c C&S |
Urinalysis with Culture and Sensitivity |
VSS |
Vital Signs Stable |
TURP |
Trans Uretheral Prostatectomy |
TAB |
Therapeutic Abortion |
VIP |
Voluntary Interruption of Pregnancy |
PNA |
Pneumonia |
ddx |
Differential Diagnosis |
abx |
Antibiotics |
bx |
Biopsy |
cx |
Culture |
Ad lib |
As much as needed |
c/o |
Complain of |
QD |
Every day |
bid |
Twice a day |
tid |
Three times a day |
qid |
Four times a day |
Q.O.D. |
Every Other Day |
Tanya Oberoi Pandya D.O., M.B.A.
| Fact Name | Description | Governing Law |
|---|---|---|
| Purpose of the Form | The Complete Physical Examination form is used to document a comprehensive health assessment of a patient. | State-specific regulations may apply. |
| Abbreviations Used | The form contains numerous medical abbreviations, such as RRR for regular rate and rhythm and NAD for no acute distress. | State-specific regulations may apply. |
| Components of the Examination | Key sections include vital signs, general appearance, cardiovascular, respiratory, abdominal, and neurological assessments. | State-specific regulations may apply. |
| Documentation Requirements | Accurate and thorough documentation is essential for patient care continuity and legal compliance. | State-specific regulations may apply. |
Filling out the Complete Physical Examination form is straightforward, but it requires attention to detail. Once you complete the form, it will be reviewed by your healthcare provider. They will use the information to assess your health and make any necessary recommendations.
What is the purpose of the Complete Physical Examination form?
The Complete Physical Examination form is used to document a comprehensive assessment of a person's health. It covers various aspects such as vital signs, general appearance, and specific examinations of different body systems. This form helps healthcare providers identify any health issues and track changes over time.
What information is included in the vital signs section?
The vital signs section includes key measurements that indicate a person's basic bodily functions. These measurements are temperature (T), heart rate (HR), respiration rate (RR), blood pressure (BP), and oxygen saturation (SPO2). Each of these indicators provides important information about a person's health status and can help identify potential medical concerns.
How are findings documented in the physical examination section?
Findings from the physical examination are documented using specific abbreviations and descriptions. For example, the general appearance may note if a person is alert and in no acute distress. Other sections, like cardiovascular or respiratory, will include terms like "regular rate and rhythm" or "clear to auscultation bilaterally." This standardized documentation helps ensure clarity and consistency in medical records.
What should I expect during a physical examination?
During a physical examination, a healthcare provider will assess various aspects of your health. They may check your vital signs, examine your heart and lungs, and assess your abdomen and extremities. You can expect questions about your medical history and any current concerns. The process is generally straightforward and aims to provide a complete picture of your health.
Incomplete Information: Failing to fill out all required sections can lead to misunderstandings or missed health issues. Ensure every section is addressed.
Incorrect Abbreviations: Using the wrong abbreviations can create confusion. Familiarize yourself with the standard abbreviations to avoid errors.
Missing Medical History: Omitting past medical history can impact the examination results. Always include relevant details about previous illnesses or surgeries.
Neglecting Current Medications: Not listing current medications can lead to potential drug interactions or misdiagnoses. Be thorough in documenting all medications.
Ignoring Allergies: Failing to mention known allergies can pose serious risks during examinations or treatments. Always highlight any allergies clearly.
Overlooking Symptoms: Downplaying or omitting symptoms may prevent proper diagnosis. Be honest and detailed about any health concerns.
Using Inconsistent Terminology: Switching terms or using non-standard language can confuse healthcare providers. Stick to commonly accepted terms for clarity.
Rushing the Process: Filling out the form hastily may lead to mistakes. Take your time to ensure accuracy and completeness.
Not Reviewing the Form: Failing to double-check the completed form can result in overlooked errors. Always review your entries before submission.
The Complete Physical Examination form is an essential document in healthcare settings, providing a comprehensive overview of a patient's health status. Alongside this form, several other documents are commonly utilized to ensure thorough patient evaluation and care. Below are four key forms that often accompany the Complete Physical Examination form.
Utilizing these documents alongside the Complete Physical Examination form enhances the quality of patient care. Each form plays a vital role in building a comprehensive understanding of the patient’s health and facilitating effective communication among healthcare providers.
The Complete Physical Examination form shares similarities with the Medical History form. Both documents aim to gather comprehensive information about a patient's health. The Medical History form focuses on past medical issues, surgeries, and family health background. It often includes details about allergies, medications, and lifestyle choices. In contrast, the Complete Physical Examination form emphasizes the current state of health, assessing vital signs and conducting a physical exam. Together, they provide a holistic view of a patient's health status.
Another document similar to the Complete Physical Examination form is the Progress Note. Progress Notes are routinely used in medical practice to track a patient’s ongoing health status and treatment progress. They include updates on symptoms, responses to treatment, and any changes in the patient's condition. While the Complete Physical Examination form is a snapshot of a patient’s health at a specific time, Progress Notes provide a continuous record that helps healthcare providers monitor improvements or declines in health over time.
The Referral Form is also akin to the Complete Physical Examination form. This document is used when a healthcare provider recommends that a patient see a specialist for further evaluation or treatment. It typically includes relevant medical history, current symptoms, and the reason for the referral. Both forms serve to communicate important health information, ensuring that specialists have the necessary background to provide appropriate care. The Referral Form, however, focuses more on the need for specialized attention rather than a comprehensive assessment.
Lastly, the Consent Form bears similarities to the Complete Physical Examination form in that both are essential for patient care. The Consent Form ensures that patients understand the procedures they will undergo, including the physical examination. It outlines potential risks and benefits, allowing patients to make informed decisions about their healthcare. While the Complete Physical Examination form documents the findings of the examination, the Consent Form confirms that the patient agrees to participate in the evaluation process, highlighting the importance of patient autonomy in medical care.
When filling out the Complete Physical Examination form, there are several important considerations to keep in mind. Here is a list of things you should and shouldn't do:
Understanding the Complete Physical Examination form is essential for both healthcare providers and patients. However, several misconceptions can lead to confusion. Here are eight common misconceptions, along with clarifications for each:
By addressing these misconceptions, patients and providers can better appreciate the significance of the Complete Physical Examination form in promoting health and wellness.
When it comes to filling out and using the Complete Physical Examination form, there are several key points to keep in mind. These tips can help ensure that the process is smooth and effective.
By keeping these key takeaways in mind, you can ensure that the Complete Physical Examination form is filled out accurately and comprehensively, providing valuable information for patient care.