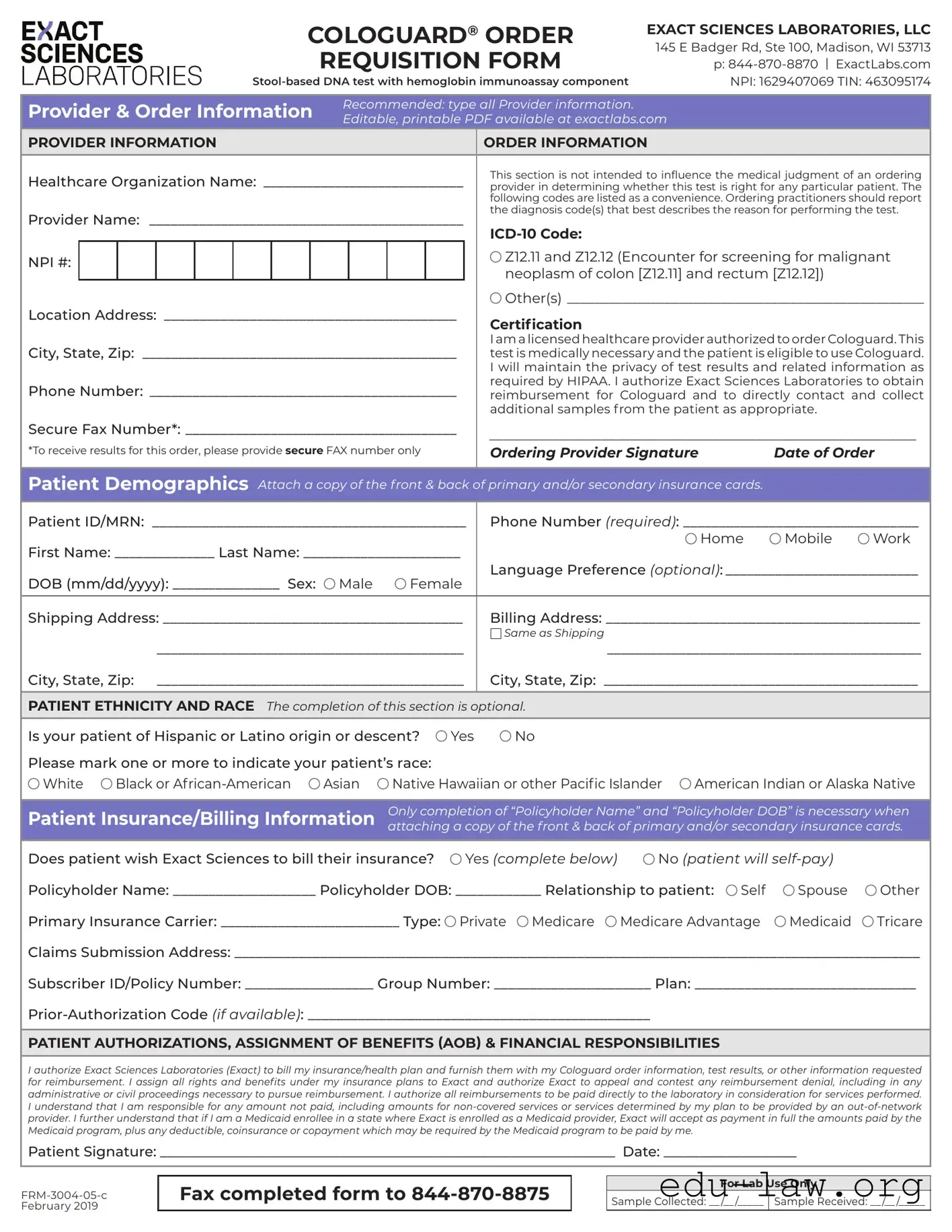
The Cologuard Order form is a crucial document for healthcare providers looking to order the Cologuard test, a stool-based DNA screening tool designed to detect colorectal cancer. This form, provided by Exact Sciences Laboratories, includes essential sections for both provider and patient information, ensuring that all necessary details are captured for a smooth testing process. Providers must fill out their information, including their name, organization, and contact details, as well as the patient's demographics, such as name, date of birth, and insurance information. The form also emphasizes the importance of medical necessity and patient eligibility, requiring the provider's signature to confirm these factors. Additionally, there are sections for patient ethnicity and race, which are optional but can aid in understanding population health trends. Lastly, the form includes authorizations for billing and financial responsibilities, making it clear who is responsible for payment and what information will be shared with insurance companies. Completing this form accurately is vital for ensuring that patients receive timely testing and results.
|
|
|
|
|
|
|
COLOGUARD® ORDER |
EXACT SCIENCES LABORATORIES, LLC |
|||||||||
|
|
|
|
|
|
|
|
|
REQUISITION FORM |
145 E Badger Rd, Ste 100, Madison, WI 53713 |
|||||||
|
|
|
|
|
|
|
|
|
|
p: |
|||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
NPI: 1629407069 TIN: 463095174 |
||||||||||
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider & Order Information |
Recommended: type all Provider information. |
|
|
||||||||||||||
Editable, printable PDF available at exactlabs.com |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
PROVIDER INFORMATION |
|
|
|
|
|
ORDER INFORMATION |
|
||||||||||
Healthcare Organization Name: _____________________________ |
This section is not intended to influence the medical judgment of an ordering |
||||||||||||||||
provider in determining whether this test is right for any particular patient. The |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
following codes are listed as a convenience. Ordering practitioners should report |
|||
Provider Name: _____________________________________________ |
the diagnosis code(s) that best describes the reason for performing the test. |
||||||||||||||||
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NPI #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Z12.11 and Z12.12 (Encounter for screening for malignant |
|||
|
|
|
|
|
|
|
|
|
|
|
|
neoplasm of colon [Z12.11] and rectum [Z12.12]) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Location Address: __________________________________________ |
Other(s)____________________________________________________ |
||||||||||||||||
Certification |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City, State, Zip: _____________________________________________ |
I am a licensed healthcare provider authorized to order Cologuard. This |
||||||||||||||||
test is medically necessary and the patient is eligible to use Cologuard. |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I will maintain the privacy of test results and related information as |
|||
Phone Number: ____________________________________________ |
required by HIPAA. I authorize Exact Sciences Laboratories to obtain |
||||||||||||||||
reimbursement for Cologuard and to directly contact and collect |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
additional samples from the patient as appropriate. |
|||
Secure Fax Number*: ______________________________________ |
_____________________________________________________________ |
||||||||||||||||
*To receive results for this order, please provide secure FAX number only |
|||||||||||||||||
Ordering Provider Signature |
Date of Order |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Demographics Attach a copy of the front & back of primary and/or secondary insurance cards.
Patient ID/MRN: ____________________________________________ |
Phone Number (required): _________________________________ |
||||||||||
First Name: ______________ Last Name: ______________________ |
|
|
Home |
Mobile |
Work |
||||||
Language Preference (optional):____________________________ |
|||||||||||
DOB (mm/dd/yyyy): _______________ Sex: |
Male |
Female |
|||||||||
|
|
|
|
|
|
||||||
Shipping Address: __________________________________________ |
Billing Address: ____________________________________________ |
||||||||||
|
|
|
|
|
Same as Shipping |
|
|
|
|
|
|
|
___________________________________________ |
____________________________________________ |
|||||||||
City, State, Zip: ___________________________________________ |
City, State, Zip: ____________________________________________ |
||||||||||
|
|
|
|
|
|
|
|||||
PATIENT ETHNICITY AND RACE The completion of this section is optional. |
|
|
|
|
|
||||||
Is your patient of Hispanic or Latino origin or descent? |
Yes |
No |
|
|
|
|
|
||||
Please mark one or more to indicate your patient’s race: |
|
|
|
|
|
|
|
||||
White |
Black or |
Asian |
Native Hawaiian or other Pacific Islander |
American Indian or Alaska Native |
|||||||
|
|
|
|
|
|||||||
Patient Insurance/Billing Information |
Only completion of “Policyholder Name” and “Policyholder DOB” is necessary when |
||||||||||
attaching a copy of the front & back of primary and/or secondary insurance cards. |
|||||||||||
|
|
|
|
|
|||||||
Does patient wish Exact Sciences to bill their insurance? |
Yes (complete below) |
No (patient will |
|
||||||||
Policyholder Name: ____________________ Policyholder DOB: ____________ Relationship to patient: |
Self |
Spouse |
Other |
||||||||
Primary Insurance Carrier: _________________________ Type: |
Private Medicare |
Medicare Advantage |
Medicaid |
Tricare |
|||||||
Claims Submission Address: ________________________________________________________________________________________________
Subscriber ID/Policy Number: __________________ Group Number: ______________________ Plan: _______________________________
PATIENT AUTHORIZATIONS, ASSIGNMENT OF BENEFITS (AOB) & FINANCIAL RESPONSIBILITIES
I authorize Exact Sciences Laboratories (Exact) to bill my insurance/health plan and furnish them with my Cologuard order information, test results, or other information requested for reimbursement. I assign all rights and benefits under my insurance plans to Exact and authorize Exact to appeal and contest any reimbursement denial, including in any administrative or civil proceedings necessary to pursue reimbursement. I authorize all reimbursements to be paid directly to the laboratory in consideration for services performed. I understand that I am responsible for any amount not paid, including amounts for
Patient Signature: _________________________________________________________________ Date: ___________________
Fax completed form to
For Lab Use Only
Sample Collected: __ /__ /_____ Sample Received: __ /__ /_____
| Fact Name | Description |
|---|---|
| Provider Information | The order form requires comprehensive provider details, including name, organization, and NPI number. |
| Test Description | Cologuard is a stool-based DNA test that includes a hemoglobin immunoassay component. |
| Patient Eligibility | The ordering provider must confirm that the test is medically necessary and that the patient qualifies for Cologuard. |
| Insurance Information | Patients can choose whether Exact Sciences should bill their insurance or if they will self-pay for the test. |
| Patient Privacy | Providers must maintain the confidentiality of test results in accordance with HIPAA regulations. |
| Authorization Requirements | The form includes sections for patient authorizations, including assignment of benefits and financial responsibilities. |
| State-Specific Forms | Different states may have specific requirements governing the use of Cologuard, based on local healthcare laws. |
Filling out the Cologuard Order form is a straightforward process that requires accurate information to ensure proper handling and billing. After completing the form, it will be submitted for processing. Follow the steps below to fill out the form correctly.
What is the Cologuard test?
Cologuard is a non-invasive stool-based DNA test that helps screen for colorectal cancer. It combines DNA analysis with a hemoglobin immunoassay component, making it a comprehensive option for early detection. This test is suitable for average-risk adults aged 45 and older.
How do I fill out the Cologuard Order form?
To complete the Cologuard Order form, provide all necessary provider information, including your name, organization, and contact details. Fill in the patient's demographics, such as their name, date of birth, and insurance information. Ensure that you sign and date the form to authorize the test. If you need assistance, an editable PDF version is available on the Exact Labs website.
What insurance information is required on the form?
When filling out the insurance section, you need to provide the policyholder's name and date of birth if you're attaching copies of insurance cards. Include the primary insurance carrier, type of insurance, and any relevant policy numbers. This information helps facilitate billing and reimbursement processes.
Can patients self-pay for the Cologuard test?
Yes, patients have the option to self-pay for the Cologuard test. If a patient chooses this route, they should select “No” in the billing section of the form. This allows them to bypass insurance claims and pay directly for the test.
What happens to my insurance information after submission?
Your insurance information is used solely for billing purposes. Exact Sciences Laboratories will keep your data confidential and will handle it in compliance with HIPAA regulations. This ensures that your test results and related information remain private.
How do I authorize billing to my insurance?
By signing the Cologuard Order form, you authorize Exact Sciences to bill your insurance for the test. This includes giving them permission to share necessary information with your insurance provider for reimbursement. It’s important to read the authorization section carefully before signing.
What if my insurance denies the claim?
If your insurance denies the claim, Exact Sciences has the right to appeal the decision on your behalf. You will remain responsible for any amounts not covered by your insurance, including services deemed out-of-network or non-covered. Always stay informed about your plan's coverage details.
How do I submit the completed Cologuard Order form?
Once you have filled out the form completely, fax it to 844-870-8875. Ensure that all required sections are completed to avoid any delays in processing. Keep a copy of the form for your records, as it may be useful for future reference.
Incomplete Provider Information: Failing to fill out all required fields, such as the provider's name, organization, and contact information, can lead to delays in processing the order. Ensure that every section is completed accurately.
Incorrect Diagnosis Codes: Using the wrong ICD-10 codes can result in claim denials. It is crucial to select the appropriate codes that correspond to the patient's condition and the reason for the test.
Neglecting Patient Demographics: Omitting essential patient information, like the date of birth or contact number, can hinder communication and affect the test's outcome. Always double-check that all demographic fields are filled out correctly.
Insurance Information Errors: Providing inaccurate insurance details, such as the policyholder's name or relationship to the patient, can lead to billing issues. Verify that all insurance information is correct and complete before submission.
The Cologuard Order form is an essential document for healthcare providers when ordering the stool-based DNA test for patients. However, several other forms and documents often accompany this order to ensure a smooth process from initiation to billing. Below is a list of these related documents, each serving a specific purpose.
Each of these documents plays a crucial role in the overall process of ordering and administering the Cologuard test. Properly completing and submitting them helps streamline the workflow and ensures compliance with legal and medical standards.
The Cologuard Order form shares similarities with the Lab Requisition Form, commonly used in various healthcare settings. Both documents serve as a means for healthcare providers to request laboratory tests for their patients. They include sections for provider and patient information, ensuring that the laboratory has all necessary details to process the request efficiently. Additionally, both forms require the provider’s signature, affirming that the test is medically necessary and that patient privacy will be maintained.
Another document akin to the Cologuard Order form is the Prescription Pad. Like the Cologuard form, a prescription pad contains sections for patient information and the healthcare provider's details. It allows providers to specify the medication or test they are prescribing, ensuring clarity for pharmacists or laboratories. Both documents emphasize the importance of the provider’s authorization, which is crucial for legal and medical accountability.
The Patient Intake Form is also similar in nature to the Cologuard Order form. This document gathers essential information about the patient, including demographics and medical history. Both forms require personal data to ensure the correct identification of the patient. While the Patient Intake Form focuses more on the patient's background, the Cologuard Order form emphasizes the test specifics and billing information.
In the realm of insurance, the Authorization for Release of Information form bears resemblance to the Cologuard Order form. Both documents involve patient consent and often require signatures to ensure compliance with privacy laws. The Cologuard Order form explicitly states that the provider will maintain patient confidentiality, while the Authorization for Release of Information allows for the sharing of medical information with third parties, such as insurance companies.
The Medical History Form is another document that parallels the Cologuard Order form. Both forms collect vital patient information, which is essential for making informed medical decisions. While the Medical History Form focuses on the patient’s past health issues, the Cologuard Order form is more focused on the current need for testing and the associated billing aspects.
Similarly, the Consent Form for Medical Procedures shares characteristics with the Cologuard Order form. Both require the patient’s signature to indicate informed consent, ensuring that patients understand the procedures or tests being conducted. While the Consent Form is typically used for surgical or invasive procedures, the Cologuard form addresses non-invasive testing, yet both emphasize patient rights and responsibilities.
The Insurance Claim Form is another document that shares similarities with the Cologuard Order form, particularly in the context of billing and reimbursement. Both forms require detailed information about the patient’s insurance coverage and often necessitate the provider’s signature. The Cologuard Order form includes sections for insurance information to facilitate billing, much like the Insurance Claim Form, which is used to request payment from insurance companies.
The Referral Form is also comparable to the Cologuard Order form. Both documents serve as a communication tool between healthcare providers, ensuring that patients receive appropriate tests or specialist care. The Cologuard Order form specifies the need for a stool-based DNA test, while a Referral Form typically outlines the reason for referring a patient to another provider, thus fostering continuity of care.
Lastly, the Patient Authorization Form for Treatment is similar to the Cologuard Order form in that both require patient consent for the healthcare provider to proceed with specific actions. This form ensures that patients are aware of and agree to the tests or treatments being proposed. The Cologuard Order form emphasizes the necessity of obtaining patient authorization for billing and test processing, aligning with the principles of informed consent found in the Patient Authorization Form for Treatment.
When filling out the Cologuard Order form, it's important to follow specific guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn’t do:
Understanding the Cologuard Order form is crucial for both healthcare providers and patients. Here are six common misconceptions:
Addressing these misconceptions can help ensure a smoother process for both providers and patients when using the Cologuard Order form.
When filling out and using the Cologuard Order form, it is essential to keep the following key points in mind: