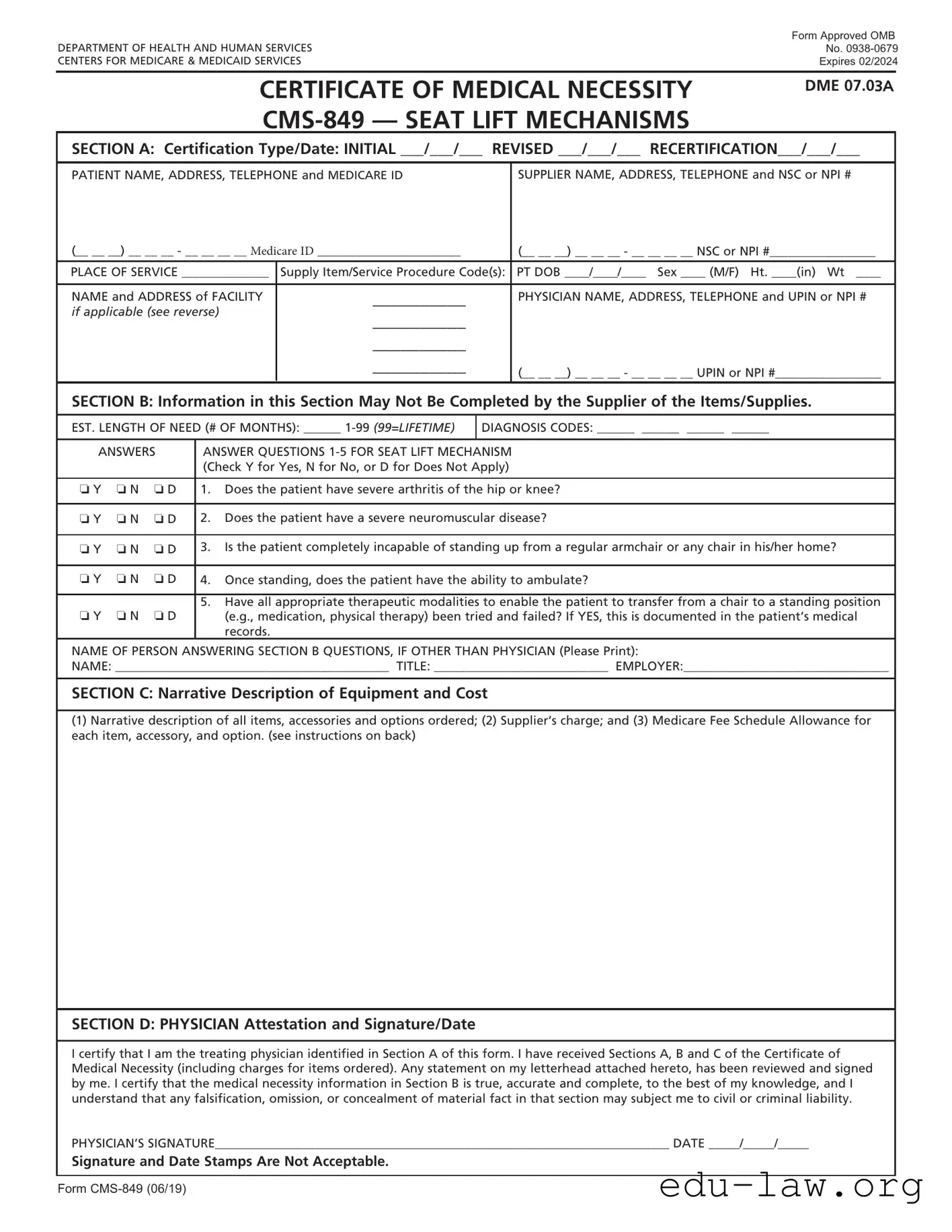
The CMS 849 form, officially known as the Certificate of Medical Necessity for Seat Lift Mechanisms, plays a crucial role in the Medicare reimbursement process for durable medical equipment (DME). This form is designed to document the medical necessity of seat lift mechanisms, which assist patients who struggle to rise from a seated position due to various health conditions. It consists of several sections that require specific information, including patient details, supplier information, and physician certification. Sections A and B focus on patient demographics and clinical assessments, while Section C outlines the equipment description and associated costs. The form concludes with the physician's attestation in Section D, confirming the accuracy of the information provided and the medical necessity of the equipment for the patient. Proper completion of the CMS 849 is essential for securing Medicare coverage, ensuring that patients receive the support they need to enhance their mobility and independence.
|
Form Approved OMB |
|
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
No. |
|
CENTERS FOR MEDICARE & MEDICAID SERVICES |
Expires 02/2024 |
|
|
|
|
CERTIFICATE OF MEDICAL NECESSITY
DME 07.03A
SECTION A: Certification Type/Date: INITIAL ___/___/___ REVISED ___/___/___ RECERTIFICATION___/___/___
PATIENT NAME, ADDRESS, TELEPHONE and MEDICARE ID |
SUPPLIER NAME, ADDRESS, TELEPHONE and NSC or NPI # |
(__ __ __) __ __ __ - __ __ __ __ Medicare ID _______________________ |
(__ __ __) __ __ __ - __ __ __ __ NSC or NPI #_________________ |
|
PLACE OF SERVICE ______________ |
Supply Item/Service Procedure Code(s): |
PT DOB ____/____/____ Sex ____ (M/F) Ht. ____(in) Wt ____ |
|
|
|
NAME and ADDRESS of FACILITY |
__________ |
PHYSICIAN NAME, ADDRESS, TELEPHONE and UPIN or NPI # |
if applicable (see reverse) |
__________ |
|
|
|
|
|
__________ |
|
|
__________ |
(__ __ __) __ __ __ - __ __ __ __ UPIN or NPI #_________________ |
|
|
|
SECTION B: Information in this Section May Not Be Completed by the Supplier of the Items/Supplies.
EST. LENGTH OF NEED (# OF MONTHS): ______
DIAGNOSIS CODES: ______ ______ ______ ______
ANSWERS |
ANSWER QUESTIONS |
|||
|
|
|
(Check Y for Yes, N for No, or D for Does Not Apply) |
|
|
|
|
|
|
o Y |
o N |
o D |
1. |
Does the patient have severe arthritis of the hip or knee? |
|
|
|
|
|
o Y |
o N |
o D |
2. |
Does the patient have a severe neuromuscular disease? |
|
|
|
|
|
o Y |
o N |
o D |
3. |
Is the patient completely incapable of standing up from a regular armchair or any chair in his/her home? |
|
|
|
|
|
o Y |
o N |
o D |
4. |
Once standing, does the patient have the ability to ambulate? |
5.Have all appropriate therapeutic modalities to enable the patient to transfer from a chair to a standing position
o Y o N o D |
(e.g., medication, physical therapy) been tried and failed? If YES, this is documented in the patient’s medical |
|
records. |
NAME OF PERSON ANSWERING SECTION B QUESTIONS, IF OTHER THAN PHYSICIAN (Please Print):
NAME: ____________________________________________ TITLE: ____________________________ EMPLOYER:_________________________________
SECTION C: Narrative Description of Equipment and Cost
(1)Narrative description of all items, accessories and options ordered; (2) Supplier’s charge; and (3) Medicare Fee Schedule Allowance for each item, accessory, and option. (see instructions on back)
SECTION D: PHYSICIAN Attestation and Signature/Date
I certify that I am the treating physician identified in Section A of this form. I have received Sections A, B and C of the Certificate of Medical Necessity (including charges for items ordered). Any statement on my letterhead attached hereto, has been reviewed and signed by me. I certify that the medical necessity information in Section B is true, accurate and complete, to the best of my knowledge, and I understand that any falsification, omission, or concealment of material fact in that section may subject me to civil or criminal liability.
PHYSICIAN’S SIGNATURE_________________________________________________________________________ DATE _____/_____/_____
Signature and Date Stamps Are Not Acceptable.
Form

INSTRUCTIONS FOR COMPLETING THE CERTIFICATE OF MEDICAL NECESSITY
FOR SEAT LIFT MECHANISMS
SECTION A: |
(May be completed by the supplier) |
CERTIFICATION |
If this is an initial certification for this patient, indicate this by placing date (MM/DD/YY) needed initially in the space TYPE/ |
DATE: |
marked “INITIAL.” If this is a revised certification (to be completed when the physician changes the order, based on the |
|
patient’s changing clinical needs), indicate the initial date needed in the space marked “INITIAL,” and indicate the |
|
recertification date in the space marked “REVISED.” If this is a recertification, indicate the initial date needed in the |
|
space marked “INITIAL,” and indicate the recertification date in the space marked “RECERTIFICATION.” Whether |
|
submitting a REVISED or a RECERTIFIED CMN, be sure to always furnish the INITIAL date as well as the REVISED or |
|
RECERTIFICATION date. |
PATIENT |
Indicate the patient’s name, permanent legal address, telephone number and his/her Medicare ID as it appears on his/her |
INFORMATION: |
Medicare card and on the claim form. |
SUPPLIER |
Indicate the name of your company (supplier name), address and telephone number along with the Medicare Supplier |
INFORMATION: |
Number assigned to you by the National Supplier Clearinghouse (NSC) or applicable National Provider Identifier (NPI). If |
|
using the NPI Number, indicate this by using the qualifier XX followed by the |
|
e.g. NSC number, use the qualifier 1C followed by the |
PLACE OF SERVICE: |
Indicate the place in which the item is being used, i.e., patient’s home is 12, skilled nursing facility (SNF) is 31, End |
|
Stage Renal Disease (ESRD) facility is 65, etc. Refer to the DMERC supplier manual for a complete list. |
FACILITY NAME: |
If the place of service is a facility, indicate the name and complete address of the facility. |
SUPPLY ITEM/SERVICE |
List all procedure codes for items ordered. Procedure codes that do not require certification should not be listed |
PROCEDURE CODE(S): |
on the CMN. |
PATIENT DOB, HEIGHT, |
Indicate patient’s date of birth (MM/DD/YY) and sex (male or female); height in inches and weight in pounds, if requested. |
WEIGHT AND SEX: |
|
PHYSICIAN NAME, |
Indicate the PHYSICIAN’S name and complete mailing address. |
ADDRESS: |
|
PHYSICIAN |
Accurately indicate the treating physician’s Unique Physician Identification Number (UPIN) or applicable National |
INFORMATION: |
Provider Identifier (NPI). If using the NPI Number, indicate this by using the qualifier XX followed by the |
|
If using UPIN number, use the qualifier 1G followed by the |
PHYSICIAN’S |
Indicate the telephone number where the physician can be contacted (preferably where records would be accessible |
TELEPHONE NO: |
pertaining to this patient) if more information is needed. |
SECTION B: |
(May not be completed by the supplier. While this section may be completed by a |
|
Physician employee, it must be reviewed, and the CMN signed (in Section D) by the treating practitioner.) |
EST. LENGTH OF NEED: |
Indicate the estimated length of need (the length of time the physician expects the patient to require use of the ordered |
|
item) by filling in the appropriate number of months. If the patient will require the item for the duration of his/her life, |
|
then enter “99”. |
DIAGNOSIS CODES: |
In the first space, list the diagnosis code that represents the primary reason for ordering this item. List any additional |
|
diagnosis codes that would further describe the medical need for the item (up to 4 codes). |
QUESTION SECTION: |
This section is used to gather clinical information to help Medicare determine the medical necessity for the item(s) |
|
being ordered. Answer each question which applies to the items ordered, checking “Y” for yes, “N” for no, or “D” for |
|
does not apply. |
NAME OF PERSON |
If a clinical professional other than the treating physician (e.g., home health nurse, physical therapist, dietician) or a |
ANSWERING SECTION B |
physician employee answers the questions of Section B, he/she must print his/her name, give his/her professional title |
QUESTIONS: |
and the name of his/her employer where indicated. If the physician is answering the questions, this space may be |
|
left blank. |
SECTION C: |
(To be completed by the supplier) |
NARRATIVE |
Supplier gives (1) a narrative description of the item(s) ordered, as well as all options, accessories, supplies and drugs; |
DESCRIPTION OF |
(2) the supplier’s charge for each item(s), options, accessories, supplies and drugs; and (3) the Medicare fee schedule |
EQUIPMENT & COST: |
allowance for each item(s), options, accessories, supplies and drugs, if applicable. |
SECTION D: |
(To be completed by the physician) |
PHYSICIAN |
The physician’s signature certifies (1) the CMN which he/she is reviewing includes Sections A, B, C and D; (2) the |
ATTESTATION: |
answers in Section B are correct; and (3) the |
PHYSICIAN SIGNATURE |
After completion and/or review by the physician of Sections A, B and C, the physician’s must sign and date the CMN in |
AND DATE: |
Section D, verifying the Attestation appearing in this Section. The physician’s signature also certifies the items ordered |
|
are medically necessary for this patient. |
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
DO NOT SUBMIT CLAIMS TO THIS ADDRESS. Please see http://www.medicare.gov/ for information on claim filing.
Form
| Fact Name | Description |
|---|---|
| Form Purpose | The CMS-849 form is used to certify the medical necessity of seat lift mechanisms for patients who require assistance in standing from a seated position. |
| Expiration Date | This form is approved by the Office of Management and Budget (OMB) and is set to expire in February 2024. |
| Sections Overview | The form consists of several sections, including patient information, certification type, medical necessity questions, and physician attestation. |
| State-Specific Laws | In California, the governing law for medical necessity forms is found in the California Code of Regulations, Title 22, Section 51000. |
| Physician's Responsibility | The physician must review and sign the form, confirming that the information provided is accurate and complete, thereby attesting to the medical necessity of the equipment. |
Completing the CMS 849 form is an essential step in ensuring that a patient receives the necessary seat lift mechanisms through Medicare. The process requires careful attention to detail, as accurate information will facilitate the approval of medical necessity. Below are the steps to effectively fill out the form.
Once the form is completed, it should be submitted according to the guidelines provided by Medicare. Ensuring that all sections are accurately filled out will help in the timely approval of the necessary equipment for the patient.
What is the purpose of the CMS 849 form?
The CMS 849 form, also known as the Certificate of Medical Necessity for Seat Lift Mechanisms, is used to document the medical necessity for a seat lift mechanism for patients. It ensures that the equipment is justified based on the patient's medical condition and needs. This form must be completed by a physician and is crucial for Medicare reimbursement.
Who is responsible for filling out the different sections of the CMS 849 form?
Sections A and C can be completed by the supplier of the equipment, while Section B must be answered by a qualified healthcare professional, typically the treating physician. The physician must also review and sign Section D to certify the accuracy of the information provided.
What information is required in Section B of the CMS 849 form?
Section B gathers clinical information to support the medical necessity of the seat lift mechanism. It includes questions about the patient's condition, such as whether they have severe arthritis or a neuromuscular disease. The physician or qualified professional must answer these questions accurately, indicating "Yes," "No," or "Does Not Apply" for each question.
How does a physician certify the information on the CMS 849 form?
In Section D, the physician must sign and date the form, confirming that they have reviewed all sections and that the information is true and complete. This signature indicates that the physician believes the seat lift mechanism is medically necessary for the patient based on the information provided in Sections A, B, and C.
Incomplete Patient Information: One of the most common mistakes is failing to provide complete patient details. This includes the patient’s full name, address, telephone number, and Medicare ID. Missing any of this information can lead to delays or denials of claims.
Incorrect Certification Dates: Applicants often mix up the certification types and dates. It's crucial to accurately indicate whether the form is for an initial certification, a revision, or a recertification. Each type requires specific dates to be filled in, and mistakes here can complicate the approval process.
Failure to Answer Section B Questions: Section B is vital for establishing medical necessity. Some individuals neglect to answer all questions or provide vague responses. Each question must be answered clearly with “Y,” “N,” or “D” to ensure that Medicare can assess the need for the seat lift mechanism appropriately.
Omitting Required Signatures: A common oversight is not securing the physician's signature in Section D. This signature is essential for certifying the information provided in the form. Without it, the form is incomplete and cannot be processed.
Inaccurate Narrative Description: In Section C, the narrative description must accurately reflect the items ordered, including all accessories and options. Failing to provide a detailed and precise description can lead to misunderstandings and potential claim denials.
The CMS 849 form, known as the Certificate of Medical Necessity for Seat Lift Mechanisms, is essential for obtaining coverage for specific medical equipment. Several other documents and forms often accompany the CMS 849 to ensure compliance with Medicare requirements and facilitate the claims process. The following is a list of commonly used forms and documents related to the CMS 849.
Each of these documents plays a vital role in the process of obtaining Medicare coverage for seat lift mechanisms. Properly completing and submitting them can help ensure that patients receive the necessary equipment without unnecessary delays.
The CMS-1500 form is often compared to the CMS-849 because both serve as essential documents for billing Medicare and other insurance programs. The CMS-1500 is primarily used by healthcare providers to submit claims for services rendered to patients, while the CMS-849 specifically addresses the medical necessity of durable medical equipment, like seat lift mechanisms. Both forms require detailed patient information, including diagnosis codes and provider information, ensuring that the services or items billed are justified and meet Medicare's criteria for coverage.
Another document similar to the CMS-849 is the Certificate of Medical Necessity (CMN) for other types of durable medical equipment, such as wheelchairs or oxygen equipment. Like the CMS-849, this CMN requires a physician's certification that the equipment is medically necessary for the patient. Both forms include sections for patient details, diagnosis codes, and a narrative description of the equipment, emphasizing the need for thorough documentation to support the claim for reimbursement from Medicare.
The Prior Authorization Request form is also comparable to the CMS-849 in that it is used to obtain approval from Medicare before providing certain medical services or equipment. This form, like the CMS-849, requires detailed patient information and clinical justification for the requested service or item. Both documents aim to ensure that the items or services are medically necessary and meet specific criteria set by Medicare, thereby streamlining the approval process and reducing the chances of claim denials.
Lastly, the Advanced Beneficiary Notice (ABN) shares similarities with the CMS-849, as both documents inform patients about their potential financial responsibilities for services that may not be covered by Medicare. While the CMS-849 focuses on establishing medical necessity for specific equipment, the ABN is used when a provider believes that a service may not be reimbursed. Both documents require clear communication between the provider and the patient, ensuring that patients are aware of their rights and responsibilities regarding their healthcare services.
When filling out the CMS 849 form, it is essential to follow specific guidelines to ensure accuracy and compliance. Below is a list of things you should and shouldn't do.
Understanding the CMS 849 form can be challenging, and several misconceptions often arise. Here are nine common misunderstandings:
When filling out the CMS 849 form, there are several important points to keep in mind. Here are some key takeaways:
Following these guidelines will help ensure that the CMS 849 form is completed correctly, facilitating a smoother approval process for the necessary medical equipment.