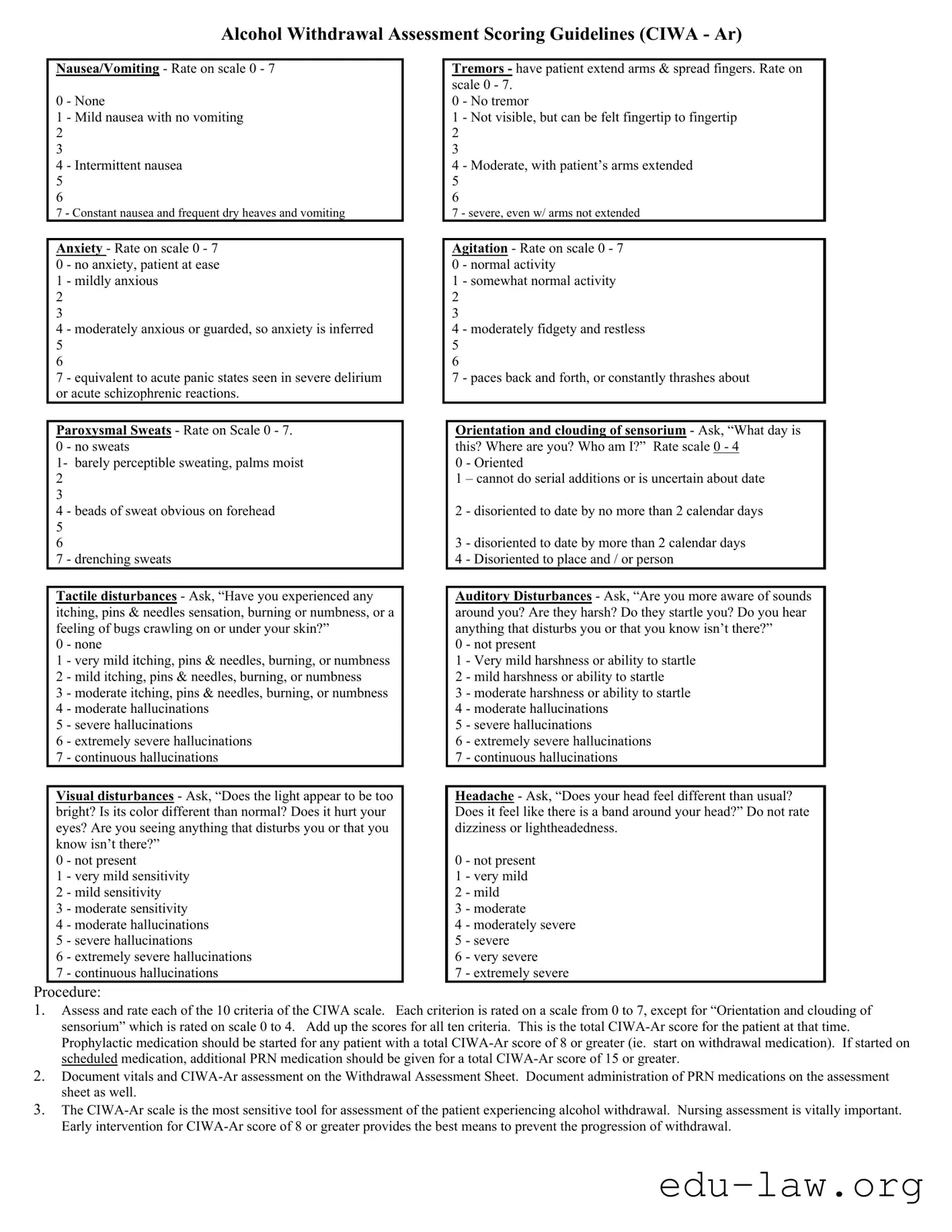
The CIWA-Ar form, or Clinical Institute Withdrawal Assessment for Alcohol, serves as a crucial tool in assessing the severity of alcohol withdrawal symptoms in patients. This assessment is particularly vital for healthcare providers, as it guides decisions regarding the initiation of treatment and the administration of medications. The form evaluates ten distinct criteria, including nausea and vomiting, anxiety, tremors, and various sensory disturbances, each rated on a specific scale. For instance, nausea can range from none to constant, while anxiety levels can shift from being at ease to experiencing acute panic. Additionally, the CIWA-Ar takes into account the patient's orientation and clouding of sensorium, as well as auditory and visual disturbances, providing a comprehensive picture of the patient's condition. The scoring system is designed to facilitate early intervention, with a total score of 8 or higher indicating the need for prophylactic medication. This proactive approach is essential in preventing the progression of withdrawal symptoms, ultimately ensuring better outcomes for individuals undergoing alcohol detoxification.
Alcohol Withdrawal Assessment Scoring Guidelines (CIWA - Ar)
Nausea/Vomiting - Rate on scale 0 - 7
0 - None
1 - Mild nausea with no vomiting
2
3
4 - Intermittent nausea
5
6
7 - Constant nausea and frequent dry heaves and vomiting
Anxiety - Rate on scale 0 - 7
0 - no anxiety, patient at ease
1 - mildly anxious
2
3
4 - moderately anxious or guarded, so anxiety is inferred 5 6
7 - equivalent to acute panic states seen in severe delirium or acute schizophrenic reactions.
Paroxysmal Sweats - Rate on Scale 0 - 7.
0 - no sweats
1- barely perceptible sweating, palms moist
2
3
4 - beads of sweat obvious on forehead
5
6
7 - drenching sweats
Tactile disturbances - Ask, “Have you experienced any itching, pins & needles sensation, burning or numbness, or a feeling of bugs crawling on or under your skin?”
0 - none
1 - very mild itching, pins & needles, burning, or numbness 2 - mild itching, pins & needles, burning, or numbness
3 - moderate itching, pins & needles, burning, or numbness 4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Visual disturbances - Ask, “Does the light appear to be too bright? Is its color different than normal? Does it hurt your eyes? Are you seeing anything that disturbs you or that you know isn’t there?”
0 - not present
1 - very mild sensitivity
2 - mild sensitivity
3 - moderate sensitivity
4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Tremors - have patient extend arms & spread fingers. Rate on scale 0 - 7.
0 - No tremor
1 - Not visible, but can be felt fingertip to fingertip 2 3
4 - Moderate, with patient’s arms extended
5
6
7 - severe, even w/ arms not extended
Agitation - Rate on scale 0 - 7 0 - normal activity
1 - somewhat normal activity
2
3
4 - moderately fidgety and restless
5
6
7 - paces back and forth, or constantly thrashes about
Orientation and clouding of sensorium - Ask, “What day is this? Where are you? Who am I?” Rate scale 0 - 4
0 - Oriented
1 – cannot do serial additions or is uncertain about date
2 - disoriented to date by no more than 2 calendar days
3 - disoriented to date by more than 2 calendar days 4 - Disoriented to place and / or person
Auditory Disturbances - Ask, “Are you more aware of sounds around you? Are they harsh? Do they startle you? Do you hear anything that disturbs you or that you know isn’t there?”
0 - not present
1 - Very mild harshness or ability to startle
2 - mild harshness or ability to startle
3 - moderate harshness or ability to startle
4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Headache - Ask, “Does your head feel different than usual? Does it feel like there is a band around your head?” Do not rate dizziness or lightheadedness.
0 - not present
1 - very mild
2 - mild
3 - moderate
4 - moderately severe
5 - severe
6 - very severe
7 - extremely severe
Procedure:
1.Assess and rate each of the 10 criteria of the CIWA scale. Each criterion is rated on a scale from 0 to 7, except for “Orientation and clouding of sensorium” which is rated on scale 0 to 4. Add up the scores for all ten criteria. This is the total
2.Document vitals and
3.The
|
Assessment Protocol |
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
a. Vitals, Assessment Now. |
|
|
Time |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
b. If initial score 8 repeat q1h x 8 hrs, then |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
if stable q2h x 8 hrs, then if stable q4h. |
|
Pulse |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
c. If initial score < 8, assess q4h x 72 hrs. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
RR |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
If score < 8 for 72 hrs, d/c assessment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
If score 8 at any time, go to (b) above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
O2 sat |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
d. If indicated, (see indications below) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
administer prn medications as ordered and |
|
BP |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
record on MAR and below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Assess and rate each of the following |
Refer to reverse for detailed instructions in use of the |
|||||||||||||||||
|
Nausea/vomiting (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- none; 1 - mild nausea ,no vomiting; 4 - intermittent nausea; |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
7 |
- constant nausea , frequent dry heaves & vomiting. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Tremors (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- no tremor; 1 - not visible but can be felt; 4 - moderate w/ arms |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
extended; 7 - severe, even w/ arms not extended. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Anxiety (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- none, at ease; 1 - mildly anxious; 4 - moderately anxious or |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
guarded; 7 - equivalent to acute panic state |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Agitation (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- normal activity; 1 - somewhat normal activity; 4 - moderately |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
fidgety/restless; 7 - paces or constantly thrashes about |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Paroxysmal Sweats (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- no sweats; |
1 - barely perceptible sweating, palms moist; |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4 |
- beads of sweat obvious on forehead; |
7 - drenching sweat |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Orientation (0 - 4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- oriented; 1 - uncertain about date; 2 - disoriented to date by no |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
more than 2 days; 3 - disoriented to date by > 2 days; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
4 - disoriented to place and / or person |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Tactile Disturbances (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- none; 1 - very mild itch, P&N, ,numbness; |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
burning, numbness; 3 - moderate itch, P&N, burning ,numbness; |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
4 |
- moderate hallucinations; 5 - severe hallucinations; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
6 – extremely severe hallucinations; 7 - continuous hallucinations |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Auditory Disturbances (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
0 |
- not present; 1 - very mild harshness/ ability to startle; 2 - mild |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
harshness, ability to startle; 3 - moderate harshness, ability to |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
startle; 4 - moderate hallucinations; 5 severe hallucinations; |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
6 |
- extremely severe hallucinations; 7 - continuous.hallucinations |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Visual Disturbances (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- not present; |
1 - very mild sensitivity; |
2 - mild sensitivity; |
|
|
|
|
|
|
|
|
|
|
|
|
||||
3 |
- moderate sensitivity; 4 - moderate hallucinations; 5 - severe |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
hallucinations; |
6 - extremely severe hallucinations; |
7 - |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
continuous hallucinations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Headache (0 - 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
0 |
- not present; 1 - very mild; 2 - mild; 3 - moderate; 4 - moderately |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
severe; 5 - severe; 6 - very severe; 7 - extremely severe |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
PRN Med: (circle one) |
|
Dose given (mg): |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Diazepam |
Lorazepam |
|
|
|
Route: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time of PRN medication administration: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Assessment of response |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
minutes after medication administered) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
RN Initials |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scale for Scoring:
Total Score =
0 – 9: absent or minimal withdrawal
10 – 19: mild to moderate withdrawal
more than 20: severe withdrawal
Indications for PRN medication:
a.Total
b.Total
Patient Identification (Addressograph)
Signature/ Title
Initials
Signature / Title
Initials
Alcohol Withdrawal Assessment Flowsheet (revised Nov 2003)
| Fact Name | Description |
|---|---|
| Purpose | The CIWA-Ar scale is designed to assess the severity of alcohol withdrawal symptoms in patients. |
| Scoring Criteria | The assessment includes ten criteria, each rated on a scale from 0 to 7, except for orientation, which is rated from 0 to 4. |
| Intervention Threshold | A total CIWA-Ar score of 8 or greater indicates the need for prophylactic medication to manage withdrawal symptoms. |
| Documentation Requirement | Healthcare providers must document the patient's vitals and CIWA-Ar assessment on the Withdrawal Assessment Sheet. |
| Importance of Early Intervention | Early intervention for patients with a CIWA-Ar score of 8 or higher is crucial to prevent the progression of withdrawal symptoms. |
| Governing Law | In the United States, the use of CIWA-Ar is governed by state-specific healthcare regulations and protocols for alcohol withdrawal management. |
Completing the CIWA-Ar form involves assessing a patient's symptoms related to alcohol withdrawal. This process includes rating various criteria and documenting the findings accurately. Following these steps will help ensure that the assessment is thorough and that the patient's needs are met effectively.
What is the CIWA-Ar form and why is it important?
The CIWA-Ar form, or Clinical Institute Withdrawal Assessment for Alcohol-Revised, is a standardized tool used to assess the severity of alcohol withdrawal symptoms in patients. This assessment is crucial because it helps healthcare providers determine the appropriate level of care and treatment needed for individuals experiencing withdrawal. By scoring various symptoms, such as nausea, anxiety, and tremors, the CIWA-Ar allows for early intervention, which can significantly reduce the risk of complications associated with alcohol withdrawal.
How is the CIWA-Ar score calculated?
The CIWA-Ar score is calculated by assessing ten specific criteria, each rated on a scale from 0 to 7, except for "Orientation and clouding of sensorium," which is rated from 0 to 4. Each symptom is evaluated based on the patient's current experience. After rating each criterion, the scores are summed to produce a total CIWA-Ar score. A score of 8 or greater indicates the need for prophylactic medication, while a score of 15 or higher may require additional PRN medication.
What symptoms are assessed using the CIWA-Ar form?
The CIWA-Ar form assesses a range of symptoms associated with alcohol withdrawal. These include nausea/vomiting, anxiety, paroxysmal sweats, tactile disturbances, visual disturbances, tremors, agitation, orientation, auditory disturbances, and headache. Each symptom is rated based on its severity, allowing healthcare providers to gauge the overall condition of the patient and make informed treatment decisions.
How often should the CIWA-Ar assessment be performed?
The frequency of CIWA-Ar assessments depends on the initial score. If the initial score is 8 or higher, assessments should be repeated every hour for up to eight hours. If the score remains stable and below 8, assessments can be done every four hours for up to 72 hours. If at any point the score rises to 8 or above, the more frequent assessment protocol should be resumed. This systematic approach helps ensure timely intervention and monitoring of the patient's condition.
What actions should be taken based on the CIWA-Ar score?
Based on the CIWA-Ar score, specific actions are recommended. A total score of 8 or higher typically warrants the initiation of withdrawal medication. If the score reaches 15 or above, additional PRN medications may be necessary. Continuous monitoring is essential, and if a patient's score exceeds 35, or if they require significant medication dosages, transfer to an intensive care unit may be considered. These actions are vital for effectively managing alcohol withdrawal and ensuring patient safety.
Inconsistent Scoring: One common mistake is not adhering to the scoring guidelines for each symptom. Each criterion has specific ratings from 0 to 7, or 0 to 4 for orientation. Skipping numbers or using arbitrary scores can lead to inaccurate assessments.
Neglecting Patient Communication: It's crucial to ask patients the right questions. Failing to engage with them about their experiences can result in missed symptoms. For instance, not asking about visual or auditory disturbances might overlook significant issues.
Ignoring the Total Score: After scoring each criterion, the total CIWA-Ar score must be calculated. Some individuals forget this step, leading to a lack of necessary interventions. A score of 8 or greater indicates the need for prophylactic medication.
Inadequate Documentation: Proper documentation is vital. Forgetting to record the CIWA-Ar assessment and vital signs can create gaps in patient care. This oversight can hinder effective monitoring and treatment adjustments over time.
The CIWA-Ar form is a critical tool for assessing alcohol withdrawal symptoms. Alongside this form, several other documents are frequently utilized to ensure comprehensive patient care. Each document serves a specific purpose in the assessment, treatment, and monitoring of patients experiencing alcohol withdrawal. Below is a list of these forms and documents.
These documents collectively enhance the management of alcohol withdrawal, allowing for accurate assessments, effective treatment, and thorough documentation. Proper use of these forms contributes significantly to patient safety and quality of care.
The CIWA-Ar form is similar to the Clinical Opiate Withdrawal Scale (COWS), which is used to assess withdrawal symptoms in patients undergoing opiate withdrawal. Both tools utilize a scoring system that evaluates specific symptoms to determine the severity of withdrawal. Just like the CIWA-Ar, the COWS includes criteria such as sweating, tremors, and anxiety, which are rated on a scale. This allows healthcare providers to monitor the patient's condition closely and intervene when necessary, ensuring a safer withdrawal process.
Another document that parallels the CIWA-Ar is the Alcohol Use Disorders Identification Test (AUDIT). While the AUDIT focuses on identifying alcohol use disorders rather than assessing withdrawal symptoms, both documents serve the purpose of improving patient care in alcohol-related contexts. The AUDIT includes questions about alcohol consumption, dependence symptoms, and alcohol-related problems. By identifying patients at risk, healthcare providers can use the CIWA-Ar to assess withdrawal symptoms and offer timely intervention.
The Minnesota Multiphasic Personality Inventory (MMPI) also shares similarities with the CIWA-Ar in its structured approach to assessing mental health conditions. While the MMPI is a psychological assessment tool, it includes scales that evaluate anxiety and mood disturbances, akin to the anxiety and agitation criteria in the CIWA-Ar. Both assessments aim to provide a comprehensive understanding of a patient's mental state, which can be crucial in managing withdrawal symptoms effectively.
The Beck Depression Inventory (BDI) is another document that aligns with the CIWA-Ar, as both assess psychological distress. The BDI specifically evaluates symptoms of depression, while the CIWA-Ar focuses on withdrawal symptoms. However, the overlap in evaluating emotional and psychological states makes both tools vital in a holistic approach to patient care. Identifying depression in patients undergoing withdrawal can help tailor treatment plans that address both physical and mental health needs.
Lastly, the Delirium Rating Scale (DRS) is comparable to the CIWA-Ar in that it assesses cognitive disturbances, particularly in patients experiencing delirium. Both scales utilize a scoring system to evaluate symptoms such as disorientation and hallucinations. By recognizing these symptoms early, healthcare providers can take appropriate measures to ensure patient safety and improve outcomes during withdrawal or delirium episodes. The DRS can complement the CIWA-Ar by providing a broader understanding of a patient's cognitive status during treatment.
When filling out the CIWA-Ar form, it is crucial to ensure accuracy and clarity. Here are six important dos and don’ts to consider:
By following these guidelines, you can help ensure that the CIWA-Ar form is filled out correctly and effectively supports the patient’s care plan.
There are several misconceptions about the CIWA-Ar form that can lead to misunderstandings regarding its use and effectiveness. The following list clarifies these misconceptions:
This is incorrect. The CIWA-Ar form is designed to assess all levels of alcohol withdrawal, including mild to moderate cases. Early intervention can help prevent the progression to more severe withdrawal symptoms.
While the CIWA-Ar score is a critical tool for assessing withdrawal severity, it should not be the sole determinant for treatment. Clinical judgment, patient history, and other factors also play important roles in treatment planning.
On the contrary, the CIWA-Ar form is widely used and recognized as one of the most sensitive tools for assessing alcohol withdrawal. It is based on established clinical criteria and has been validated in various settings.
This is misleading. The CIWA-Ar form requires trained healthcare professionals to conduct the assessment. Patients may not accurately interpret their symptoms, which could lead to incorrect scoring and treatment decisions.
The CIWA-Ar form is a critical tool used to assess the severity of alcohol withdrawal symptoms in patients. It consists of ten criteria, each rated on a specific scale, allowing healthcare providers to monitor changes effectively.
Accurate scoring is essential. Each criterion should be assessed and rated based on the patient's current symptoms. This information helps determine the need for medication and the urgency of intervention.
Documentation is vital. After completing the assessment, record the total CIWA-Ar score along with vital signs and any administered medications. This ensures continuity of care and provides essential data for future assessments.
Early intervention is key. A total CIWA-Ar score of 8 or greater indicates the need for prophylactic medication. Timely action can prevent the progression of withdrawal symptoms and improve patient outcomes.