The Case Conceptualization form serves as a critical tool for therapists, providing a structured approach to understanding clients and their presenting issues. This comprehensive document begins with an introduction to the client and significant others, detailing essential demographic information such as age, ethnicity, and relevant identifiers. It progresses to outline the presenting concerns, capturing both the client's and their family's descriptions of the problems at hand, as well as insights from broader systems like educators or legal entities. Background information is meticulously gathered, highlighting recent life changes and historical context that may influence the current situation. The form also emphasizes systemic assessment, exploring client and relational strengths, family structures, and interaction patterns. This includes examining couple dynamics, communication styles, and the impact of intergenerational patterns. Moreover, it encourages therapists to construct a genogram, visually mapping out familial relationships and relevant histories. The final sections invite reflection on client perspectives, identifying areas of agreement and disagreement, thereby fostering a collaborative therapeutic environment. Each aspect of the Case Conceptualization form not only aids in diagnosing issues but also paves the way for effective treatment planning, making it an indispensable resource in the therapeutic process.

Gehart Chapter 2 02/20/2009
42CHAPTER 2 Case Conceptualization
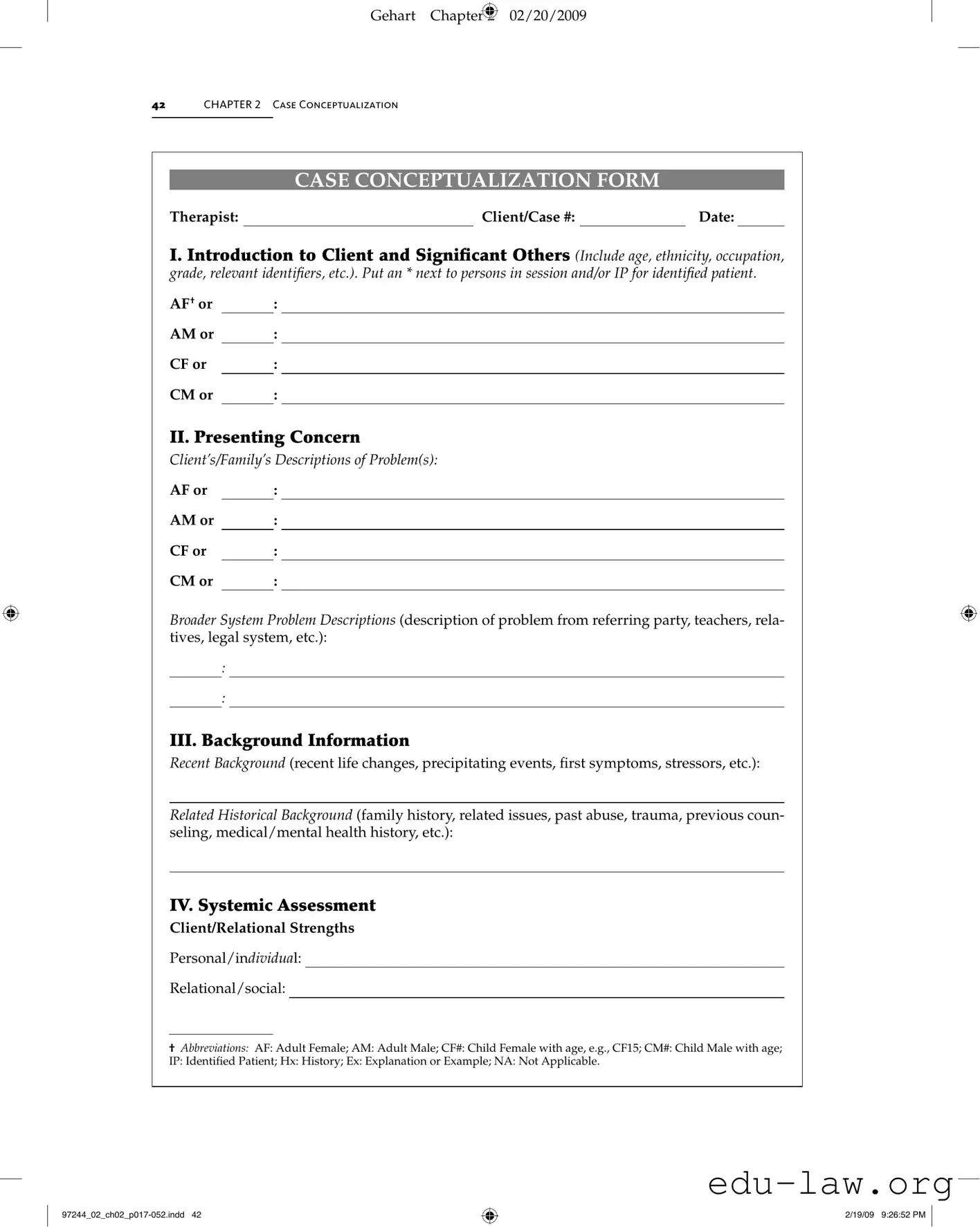
CASE CONCEPTUALIZATION FORM
Therapist: |
|
Client/Case #: |
|
Date: |
I. Introduction to Client and Signiicant Others (Include age, ethnicity, occupation, grade, relevant identii ers, etc.). Put an * next to persons in session and/or IP for identiied patient.
AF† or |
|
: |
AM or |
|
: |
CF or |
|
: |
CM or |
|
: |
II. Presenting Concern
Clients/Familys Descriptions of Problem(s):
AF or |
|
: |
AM or |
|
: |
CF or |
|
: |
CM or |
|
: |
Broader System Problem Descriptions (description of problem from referring party, teachers, rela- tives, legal system, etc.):
:
:
III. Background Information
Recent Background (recent life changes, precipitating events, irst symptoms, stressors, etc.):
Related Historical Background (family history, related issues, past abuse, trauma, previous coun- seling, medical/mental health history, etc.):
IV. Systemic Assessment
Client/Relational Strengths
Personal/individual:
Relational/social:
†Abbreviations: AF: Adult Female; AM: Adult Male; CF#: Child Female with age, e.g., CF15; CM#: Child Male with age; IP: Identiied Patient; Hx: History; Ex: Explanation or Example; NA: Not Applicable.
2/19/09 9:26:52 PM
Gehart Chapter 2 02/20/2009
Case Conceptualization Form |
43 |
|
|
|
|
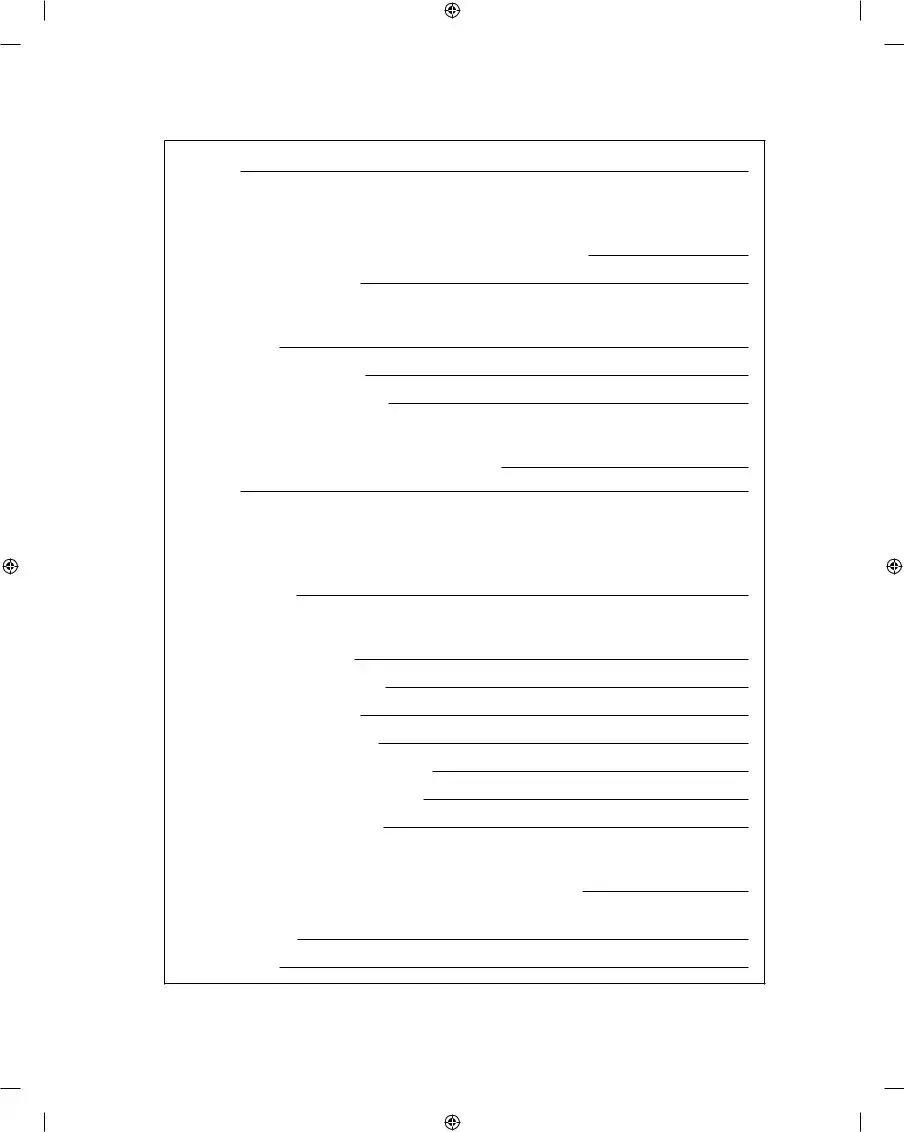
Spiritual:
Family Structure and Interaction Patterns
Couple Subsystem (to be assessed): □ Personal current □ Personal past □ Parents
Couple Boundaries: □ Clear □ Enmeshed □ Disengaged □ Other:
Rules for closeness/distance:
Couple Problem Interaction Pattern (A ⇄ B):
Start of tension:
Conlict/symptom escalation:
Return to “normal”/homeostasis:
Couple Complementary Patterns: □ Pursuer/distancer □ Over/under functioner
□Emotional/logical □ Good/bad parent □ Other: Describe:
Satirs Communication Stances:
AF: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant
AM: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant Describe dynamic:
Gottmans Divorce Indicators:
Criticism: □ AF □ AM Ex:
Defensiveness: □ AF □ AM Ex:
Contempt: □ AF □ AM Ex:
Stonewalling: □ AF □ AM Ex:
Failed repair attempts: □ AF □ AM Ex:
Not accept inluence: □ AF □ AM Ex:
Harsh startup: □ AF □ AM Ex:
Parental Subsystem: □ Family of procreation □ Family of origin
Membership in Family Subsystems: Parental: □ AF □ AM □ Other:
Is parental subsystem distinct from couple subsystem? □ Yes □ No □ NA (divorce) Sibling subsystem:
Special interest:
(continued)
2/19/09 9:26:52 PM
Gehart Chapter 2 02/20/2009
44CHAPTER 2 Case Conceptualization
(continued)
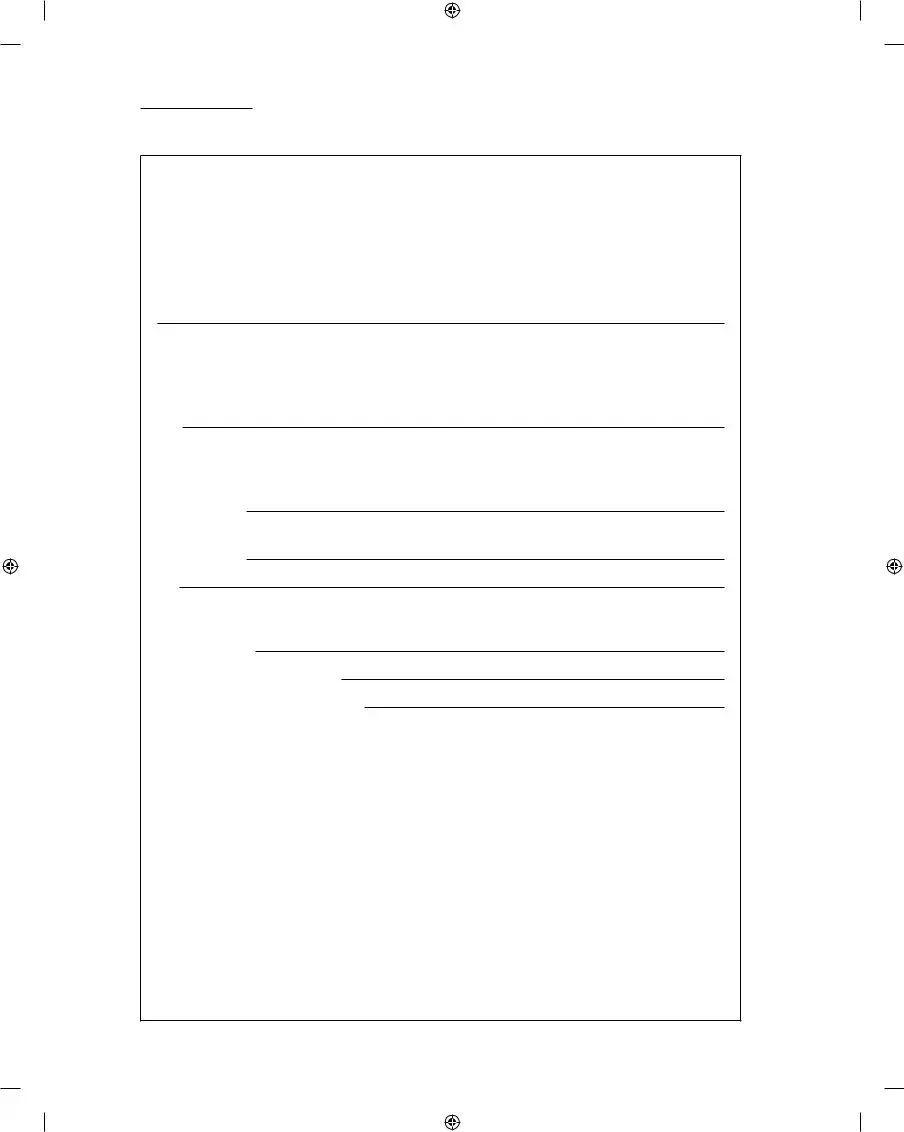
IV. Systemic Assessment
Family Structure and Interaction Patterns
Family Life Cycle Stage:
□Single adult □ Marriage □ Family with young children
□Family with adolescent children □ Launching children □ Later life Describe struggles with mastering developmental tasks in one of these stages:
Hierarchy Between Child/Parents:
AF: □ Effective □ Insuficient (permissive) □ Excessive (authoritarian) □ Inconsistent
AM: □ Effective □ Insuficient (permissive) □ Excessive (authoritarian) □ Inconsistent
Ex:
Emotional Boundaries with Children:
AF: □ Clear/balanced □ Enmeshed (reactive) □ Disengaged (disinterested)
□Other:
AM: □ Clear/balanced □ Enmeshed (reactive) □ Disengaged (disinterested)
□Other:
Ex:
Problem Interaction Pattern (A ⇄ B):
Start of tension:
Conlict/symptom escalation:
Return to “normal”/homeostasis:
Triangles/Coalitions: |
|
|
|
|
□ AF and C |
|
against AM: Ex: |
|
|
□ AM and C |
|
against AF: Ex: |
|
|
□ Other: Ex: |
|
|
|
|
Communication Stances:
AF or |
|
|
: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant |
|
AM or |
|
|
: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant |
|
CF or |
|
|
: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant |
|
CM or |
|
|
: □ Congruent □ Placator □ Blamer □ Superreasonable □ Irrelevant |
|
Ex: |
|
|
|
|
2/19/09 9:26:52 PM
Gehart Chapter 2 02/20/2009
Case Conceptualization Form |
45 |
|
|
|
|
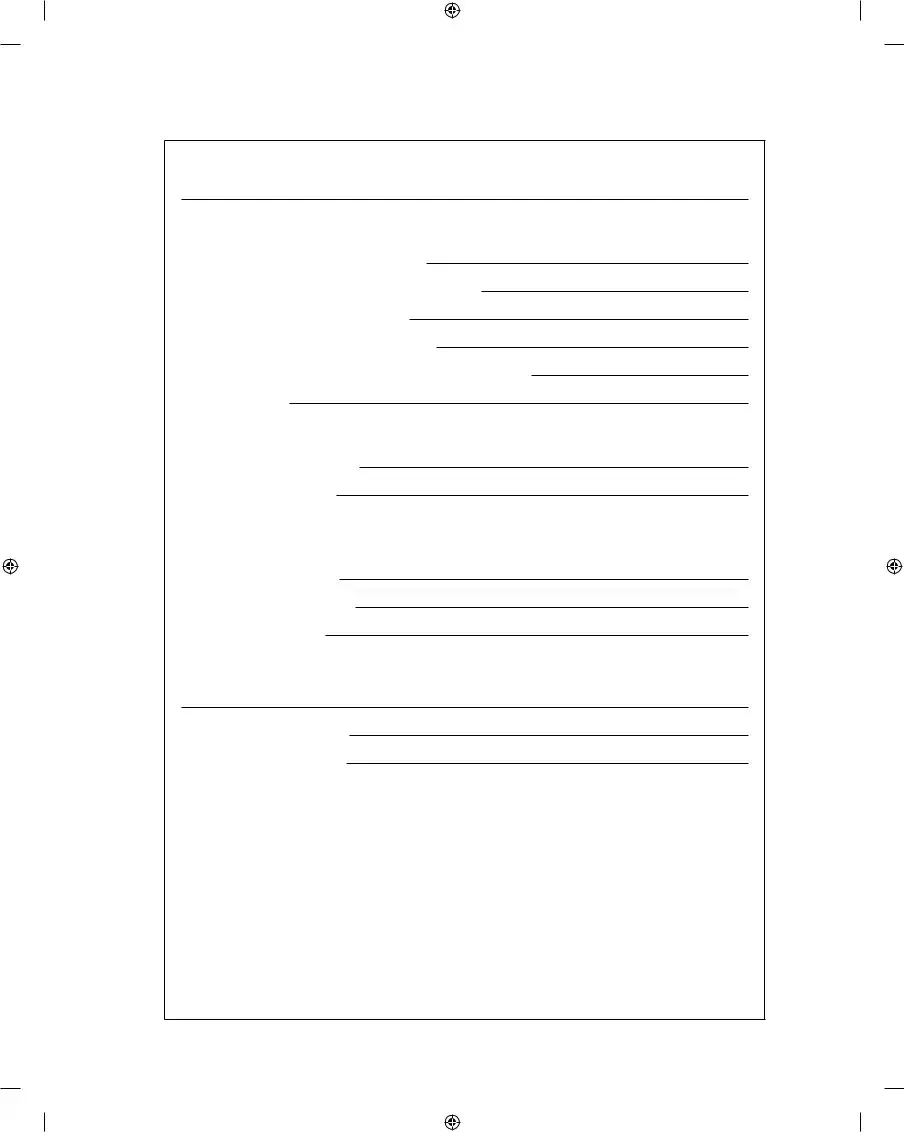
Hypothesis (Describe possible role or function of symptom in maintaining family homeostasis):
Intergenerational Patterns
Substance/alcohol abuse: □ NA □ Hx:
Sexual/physical/emotional abuse: □ NA □ Hx:
Parent/child relations: □ NA □ Hx:
Physical/mental disorders: □ NA □ Hx:
Historical incidents of presenting problem: □ NA □ Hx:
Family strengths:
Previous Solutions and Unique Outcomes
Solutions that DIDN
Solutions that DID work:
Narratives, Dominant Discourses, and Diversity
Dominant Discourses informing deinition of problem:
Cultural, ethnic, SES, etc.:
Gender, sex orientation, etc.:
Other social inluences:
Identity Narratives that have developed around problem for AF, AM, and/or CM/F:
Local or Preferred Discourses:
Other Inluential Discourses:
V. Genogram
Construct a family genogram and include all relevant information, including:
•ages, birth/death dates
•names
•relational patterns
•occupations
•medical history
•psychiatric disorders
•abuse history
Also include a couple of adjectives for persons frequently discussed in session (these should describe personal qualities and/or relational patterns, e.g., quiet, family caretaker, emotionally distant, perfectionist, helpless, etc.). Genogram should be attached to report.
(continued)
2/19/09 9:26:53 PM
Gehart Chapter 2 02/20/2009
46CHAPTER 2 Case Conceptualization
(continued)
VI. Client Perspectives
Areas of Agreement: Based on what the client(s) has(ve) said, what parts of the above assessment do they agree with or are likely to agree with?
Areas of Disagreement: What parts do they disagree with or are likely to disagree with? Why?
How do you plan to respectfully work with areas of disagreement?
©2007. Diane R. Gehart
CASE CONCEPTUALIZATION SCORING RUBRIC
The following scoring rubric describes the differences between exemplary, adequate, and deicient case conceptualizations. By closely attending to these requirements, you can hone in on what your instructors and supervisors are looking for when they grade your work.
2/19/09 9:26:53 PM |
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Case Conceptualization Form is designed to help therapists systematically assess and document client concerns, backgrounds, and systemic interactions. |
| Key Sections | The form includes sections such as Introduction to Client, Presenting Concerns, Background Information, Systemic Assessment, and Client Perspectives. |
| Usage in Therapy | Therapists use this form to create a comprehensive understanding of the client’s issues and to develop tailored treatment plans. |
| State-Specific Requirements | In some states, therapists must comply with specific laws regarding client documentation, including confidentiality and informed consent, as outlined in state licensing regulations. |
Completing the Case Conceptualization form requires careful attention to detail. Each section is designed to capture important information about the client, their concerns, and the surrounding context. Follow these steps to ensure you fill out the form accurately and comprehensively.
After completing the form, review all sections to ensure clarity and completeness. This will provide a comprehensive view of the case and support effective planning for future sessions.
What is the purpose of the Case Conceptualization form?
The Case Conceptualization form serves as a structured tool for therapists to gather and organize essential information about a client and their presenting concerns. It allows for a comprehensive understanding of the client’s background, family dynamics, and systemic interactions. By utilizing this form, therapists can develop a clearer picture of the issues at hand and formulate effective treatment strategies tailored to the client’s unique situation.
What information should be included in the introduction section?
In the introduction section, you should provide details about the client and significant others. This includes the client's age, ethnicity, occupation, and any relevant identifiers. If there are multiple individuals involved in the therapy session, mark them accordingly with an asterisk or the abbreviation for the identified patient. This foundational information sets the stage for understanding the client's context and relationships.
How do I assess presenting concerns using the form?
The form prompts you to capture both the client’s and their family's descriptions of the presenting problems. It is crucial to document these perspectives as they provide insight into how the issues are perceived by those involved. Additionally, you should include descriptions of any broader systemic problems reported by outside parties, such as teachers or legal representatives. This dual perspective helps to create a holistic view of the challenges faced.
What background information is necessary for effective case conceptualization?
Recent background information is vital, including any life changes, stressors, or precipitating events that may have influenced the client's current situation. Historical background is equally important; include family history, past traumas, and any previous counseling experiences. This comprehensive background helps identify patterns and informs the therapeutic approach.
How can I evaluate family dynamics using the form?
The form includes sections for assessing family structure and interaction patterns. You should evaluate the couple subsystem, parental hierarchy, and sibling dynamics, among other elements. Understanding these dynamics reveals how family members relate to one another and can highlight areas of strength and conflict. This information is essential for identifying potential interventions that can improve family interactions.
What is the significance of the genogram in the Case Conceptualization form?
The genogram is a visual representation of the family structure and relationships. It should include relevant details such as ages, occupations, and medical histories. By mapping out these relationships, therapists can identify patterns, strengths, and areas of concern within the family. The genogram serves as a valuable tool for both the therapist and the client, facilitating discussions about family dynamics and history.
How do I address areas of agreement and disagreement with clients?
In the client perspectives section, document areas of agreement and disagreement based on the client's feedback. Recognizing what the client agrees with helps build rapport and trust, while understanding their disagreements allows for respectful dialogue. It is important to explore the reasons behind any disagreements and to collaboratively develop strategies for addressing these differences in therapy. This approach fosters a more inclusive and effective therapeutic process.
Inadequate identification of significant others. Failing to include all relevant individuals can lead to an incomplete understanding of the client's support system. It is essential to note age, ethnicity, and relationships accurately.
Insufficient detail in presenting concerns. Clients often provide a broad overview of their issues, but specific descriptions are necessary. Without this detail, the assessment may miss critical nuances of the client's situation.
Neglecting historical background. Important life events and past experiences can significantly influence current issues. Omitting this information may result in a lack of context for understanding the client's challenges.
Failure to assess communication styles. Not evaluating the communication stances of individuals involved can overlook vital interaction patterns. This assessment is crucial for identifying potential areas of conflict or misunderstanding.
The Case Conceptualization form is a vital document for therapists and mental health professionals. It provides a comprehensive overview of the client, their presenting concerns, and the systemic factors at play. However, several other forms and documents often accompany this form to ensure a thorough understanding of the client's situation. Below are some key documents that are commonly used alongside the Case Conceptualization form.
These documents, when used in conjunction with the Case Conceptualization form, create a comprehensive framework for understanding and addressing the client's needs. Each form plays a unique role in the therapeutic process, ensuring that both the therapist and client are aligned in their approach to treatment.
The Case Conceptualization form shares similarities with the Intake Assessment form. Both documents serve to gather essential information about a client at the beginning of a therapeutic relationship. The Intake Assessment focuses on understanding the client's presenting issues, background, and personal history. It often includes questions about the client's mental health history, current stressors, and family dynamics. Like the Case Conceptualization form, it aims to create a comprehensive picture of the client's situation, which helps in formulating an effective treatment plan.
Another document that aligns closely with the Case Conceptualization form is the Treatment Plan. This document outlines the specific goals and objectives for therapy based on the client's needs and concerns. While the Case Conceptualization form provides a detailed understanding of the client's issues and the context surrounding them, the Treatment Plan translates this understanding into actionable steps. It includes measurable goals, interventions, and timelines, ensuring that both the therapist and client are on the same page regarding the therapeutic process.
The Diagnostic Assessment form also bears resemblance to the Case Conceptualization form. Both documents involve a thorough evaluation of the client's mental health status. The Diagnostic Assessment typically focuses on identifying specific mental health disorders based on established criteria, while the Case Conceptualization form takes a broader view, integrating systemic factors and relational dynamics. Both documents are essential for understanding the client's challenges and guiding treatment decisions.
Similarly, the Progress Note is another document that shares characteristics with the Case Conceptualization form. Progress Notes are used to document the ongoing therapeutic process, including client responses to interventions and changes in their condition. Like the Case Conceptualization form, Progress Notes reflect the therapist's understanding of the client's situation, but they are more focused on tracking progress over time. Both documents contribute to a comprehensive understanding of the client's journey in therapy.
Finally, the Family Assessment form aligns with the Case Conceptualization form in its focus on family dynamics and interactions. The Family Assessment gathers information about relationships, roles, and communication patterns within the family system. This information is crucial for understanding the context in which the client operates. Similarly, the Case Conceptualization form emphasizes the systemic aspects of the client's issues, making both documents vital for a holistic approach to therapy.
When filling out the Case Conceptualization form, keep the following guidelines in mind:
Understanding the Case Conceptualization form is crucial for effectively addressing client needs. However, several misconceptions can lead to confusion and hinder its proper use. Below are five common misconceptions along with explanations to clarify them.
This form is designed for a variety of professionals involved in client care, including social workers and counselors. It serves as a collaborative tool to ensure that everyone involved has a comprehensive understanding of the client's situation.
While the form may seem detailed, each section is essential for gathering relevant information about the client. This thoroughness helps in developing effective treatment plans tailored to the client's unique circumstances.
The Case Conceptualization form should be viewed as a dynamic document. As the client progresses through treatment, updates and revisions are necessary to reflect changes in their situation and needs.
In addition to identifying issues, the form emphasizes the strengths and resources of the client and their family. Recognizing these positive aspects is vital for effective treatment and empowering clients.
While it is important to collect as much information as possible, therapy can begin with incomplete data. The form is a tool for ongoing assessment, and initial sessions can help fill in gaps as the therapeutic relationship develops.
Filling out and using the Case Conceptualization form is a critical step in understanding and addressing client needs. Here are some key takeaways to keep in mind: