The CAPF 160 form, also known as the CAP Member Health History Form, is an essential document designed to ensure the safety and well-being of participants in Civil Air Patrol (CAP) activities and encampments. This confidential form gathers crucial health information that allows staff to be aware of any pre-existing medical conditions, allergies, and dietary restrictions. By accurately completing this form, individuals provide valuable insights that help staff offer appropriate support and assistance during events. The form requires personal details such as name, date of birth, and medical history, including any chronic conditions or past surgeries. It also includes sections for listing medications, allergies, and consent for treatment in emergencies. The information collected is strictly for official use and cannot be shared with unauthorized persons, emphasizing the importance of privacy and trust in the process. Completing the CAPF 160 form is a vital step in participating in CAP programs, ensuring that each member's health needs are recognized and respected.
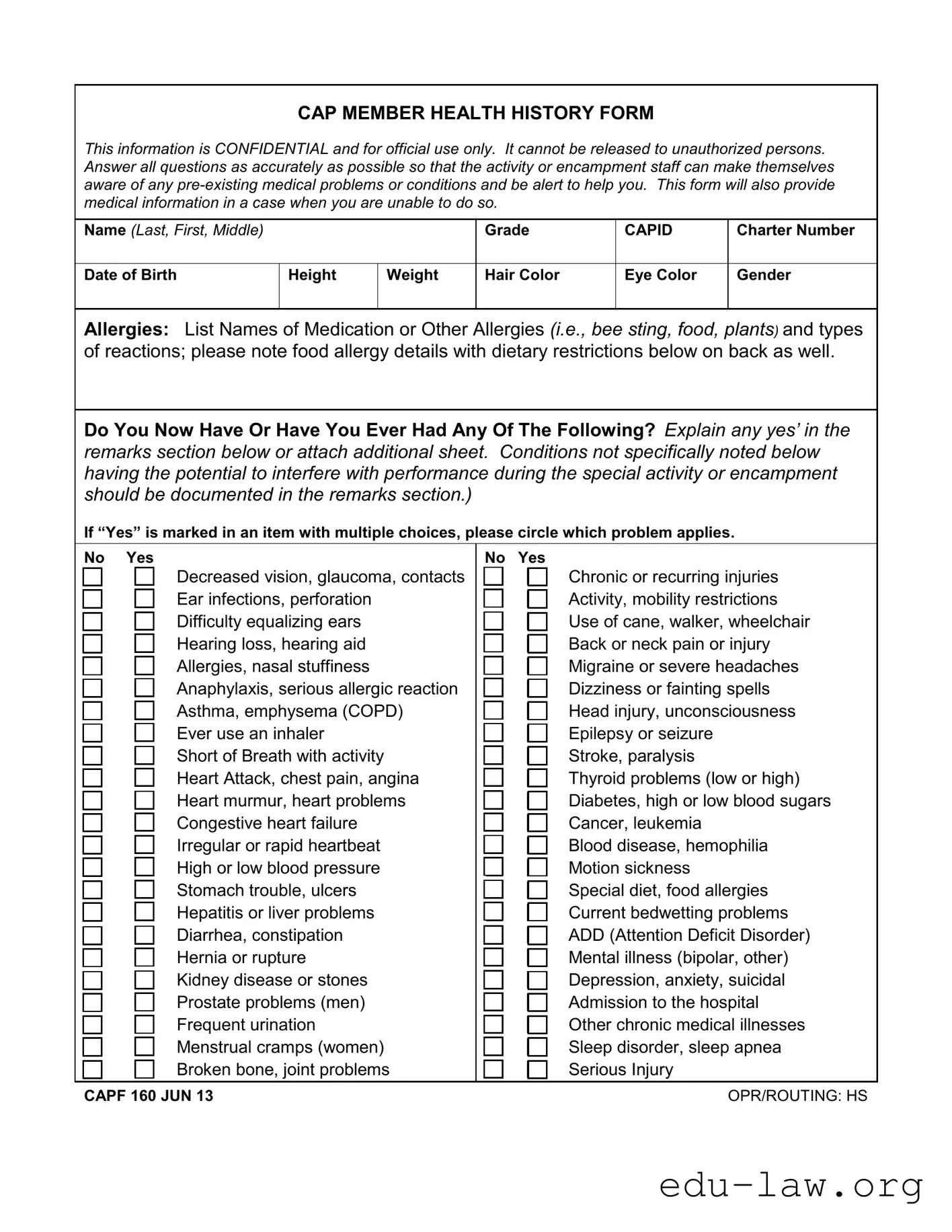
CAP MEMBER HEALTH HISTORY FORM
This information is CONFIDENTIAL and for official use only. It cannot be released to unauthorized persons. Answer all questions as accurately as possible so that the activity or encampment staff can make themselves aware of any
Name (Last, First, Middle)
Grade
CAPID
Charter Number
Date of Birth
Height
Weight
Hair Color
Eye Color
Gender
Allergies: List Names of Medication or Other Allergies (i.e., bee sting, food, plants) and types of reactions; please note food allergy details with dietary restrictions below on back as well.
Do You Now Have Or Have You Ever Had Any Of The Following? Explain any yes’ in the remarks section below or attach additional sheet. Conditions not specifically noted below having the potential to interfere with performance during the special activity or encampment should be documented in the remarks section.)
If “Yes” is marked in an item with multiple choices, please circle which problem applies.
|
No Yes |
|
No Yes |
||||||
|
|
|
|
Decreased vision, glaucoma, contacts |
|
|
|
|
Chronic or recurring injuries |
|
|
|
|
Ear infections, perforation |
|
|
|
|
Activity, mobility restrictions |
|
|
|
|
|
|
|
|
||
|
|
|
|
Difficulty equalizing ears |
|
|
|
|
Use of cane, walker, wheelchair |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hearing loss, hearing aid |
|
|
|
|
Back or neck pain or injury |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Allergies, nasal stuffiness |
|
|
|
|
Migraine or severe headaches |
|
|
|
|
|
|
|
|
||
|
|
|
|
Anaphylaxis, serious allergic reaction |
|
|
|
|
Dizziness or fainting spells |
|
|
|
|
|
|
|
|
||
|
|
|
|
Asthma, emphysema (COPD) |
|
|
|
|
Head injury, unconsciousness |
|
|
|
|
|
|
|
|
||
|
|
|
|
Ever use an inhaler |
|
|
|
|
Epilepsy or seizure |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Short of Breath with activity |
|
|
|
|
Stroke, paralysis |
|
|
|
|
|
|
|
|
||
|
|
|
|
Heart Attack, chest pain, angina |
|
|
|
|
Thyroid problems (low or high) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Heart murmur, heart problems |
|
|
|
|
Diabetes, high or low blood sugars |
|
|
|
|
|
|
|
|
||
|
|
|
|
Congestive heart failure |
|
|
|
|
Cancer, leukemia |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Irregular or rapid heartbeat |
|
|
|
|
Blood disease, hemophilia |
|
|
|
|
|
|
|
|
||
|
|
|
|
High or low blood pressure |
|
|
|
|
Motion sickness |
|
|
|
|
|
|
|
|
||
|
|
|
|
Stomach trouble, ulcers |
|
|
|
|
Special diet, food allergies |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hepatitis or liver problems |
|
|
|
|
Current bedwetting problems |
|
|
|
|
|
|
|
|
||
|
|
|
|
Diarrhea, constipation |
|
|
|
|
ADD (Attention Deficit Disorder) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hernia or rupture |
|
|
|
|
Mental illness (bipolar, other) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Kidney disease or stones |
|
|
|
|
Depression, anxiety, suicidal |
|
|
|
|
|
|
|
|
||
|
|
|
|
Prostate problems (men) |
|
|
|
|
Admission to the hospital |
|
|
|
|
|
|
|
|
||
|
|
|
|
Frequent urination |
|
|
|
|
Other chronic medical illnesses |
|
|
|
|
|
|
|
|
||
|
|
|
|
Menstrual cramps (women) |
|
|
|
|
Sleep disorder, sleep apnea |
|
|
|
|
|
|
|
|
||
|
|
|
|
Broken bone, joint problems |
|
|
|
|
Serious Injury |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
CAPF 160 JUN 13 |
OPR/ROUTING: HS |
Dietary Restrictions or Limitations (List any dietary restrictions like food allergies, diabetes,
Past Surgical History (List all surgeries including tonsils, ear tubes, appendix, gall bladder, hernia, hysterectomy, heart, heart catheterization, bone and joint and all other surgeries.)
Date Tetanus
Booster
No Td or Tdap
Date:
|
Pneumonia |
Hepatitis Vaccine |
Vaccine |
No |
No |
Date: |
Date: |
|
|
Varicella Immuni- zation/chickenpox
No
Date:
Influenza Vaccine No
Date:
Medication Information - Include supplements,
|
|
Times |
|
Any Special Dosing or Storage |
|
Tablet |
taken |
Reason for |
Instructions (i.e., as needed, with |
Name of Medication/Inhaler |
Strength |
per day |
Medication |
meals, must be refrigerated, etc.) |
1. |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
Social History
Tobacco Use (packs per day, years smoked, smokeless tobacco use)
Occupation (student or other)
Religious Preference
Remarks (Attach additional sheet if needed)
CONSENT FOR MINOR CADET PARTICIPATION, MEDICATIONS, TREATMENT
I give permission for full participation in CAP programs, subject to any limitations noted herein.
My signature below evidences my consent for my child/ward to possess and
In case of emergency, I understand every effort will be made to contact me. In the event I cannot be reached, I hereby give my permission to the licensed
___________________________ |
________________________________________________________________________________________________________ |
DATE |
SIGNATURE OF PARENT/GUARDIAN |
CAP Form 160 Reverse
| Fact Name | Details |
|---|---|
| Form Purpose | The CAPF 160 form collects essential health information for members participating in Civil Air Patrol activities. |
| Confidentiality | This form is confidential and is intended solely for official use. Unauthorized release of information is prohibited. |
| Health History | Participants must provide accurate health history, including any pre-existing conditions, to ensure safety during activities. |
| Emergency Use | The form serves as a critical resource in emergencies when a participant may be unable to communicate their medical needs. |
| Consent for Minors | Parents or guardians must sign to grant permission for their minor children to participate and receive medical treatment if necessary. |
| Medication Disclosure | Participants are required to list all medications, including over-the-counter drugs and supplements, to ensure proper care. |
| Dietary Restrictions | Any dietary restrictions or allergies must be clearly noted to accommodate individual needs during events. |
| Governing Law | This form is governed by the laws applicable to the Civil Air Patrol and may vary by state. |
Completing the CAPF 160 form is essential for ensuring that the staff is aware of any medical conditions or allergies that may affect participation in CAP activities. Follow these steps to fill out the form accurately and completely.
What is the purpose of the CAPF 160 form?
The CAPF 160 form, known as the CAP Member Health History Form, is designed to collect essential medical information from cadets participating in Civil Air Patrol activities. This form ensures that the staff is aware of any pre-existing medical conditions or allergies that could affect the cadet's participation. It serves as a vital resource in emergencies when a cadet may be unable to communicate their medical needs.
Who needs to fill out the CAPF 160 form?
All cadets participating in Civil Air Patrol programs must complete the CAPF 160 form. This requirement applies to both new and returning members. Parents or guardians must assist minors in filling out the form to ensure that all medical history, allergies, and any necessary dietary restrictions are accurately documented.
What information is required on the CAPF 160 form?
The form requires personal details such as the cadet's name, date of birth, and contact information. It also asks for specific medical history, including allergies, current medications, past surgeries, and any chronic conditions. Additionally, it includes a section for dietary restrictions and social history, which helps staff provide appropriate care and accommodations during activities.
What happens if a cadet has a medical condition that is not listed on the form?
If a cadet has a medical condition that is not specifically mentioned on the CAPF 160 form, it is crucial to document it in the remarks section. This additional information will help the activity staff understand any potential issues that could arise and ensure that appropriate measures are taken to support the cadet's health and safety during participation.
Incomplete Personal Information: Failing to provide all necessary details such as name, date of birth, and CAPID can lead to processing delays.
Ignoring Allergies: Not listing all allergies or reactions may result in serious health risks during activities. It’s crucial to detail food allergies and dietary restrictions.
Omitting Medical History: Leaving out past surgeries or chronic conditions can hinder staff from providing appropriate care. All relevant medical history should be included.
Inaccurate Medication Information: Providing incorrect details about medications, including dosage and administration instructions, can lead to dangerous situations. Ensure accuracy.
Neglecting to Explain Yes Responses: Failing to elaborate on any "Yes" answers regarding medical conditions can create confusion. Use the remarks section to clarify these points.
Missing Signature: Not signing the consent section can invalidate the form. Ensure that the parent or guardian signs and dates the form where required.
Forgetting to Update Information: Using outdated information from previous forms can lead to inaccuracies. Regularly review and update the form to reflect current health status.
The CAPF 160 form is an essential document used by the Civil Air Patrol (CAP) to gather vital health information about its members. This form ensures that staff are aware of any pre-existing medical conditions that could affect participation in activities or encampments. Alongside the CAPF 160, several other forms and documents are commonly utilized to support the health and safety of cadets. Below is a list of these documents, along with brief descriptions of their purposes.
Each of these documents plays a vital role in ensuring the safety, well-being, and proper management of CAP members. When used together with the CAPF 160, they create a comprehensive framework that supports both the health needs and participation of cadets in the Civil Air Patrol's programs.
The CAPF 160 form is similar to the Medical History Form often used in schools and camps. Just like the CAPF 160, this document collects essential health information about students or campers to ensure their safety during activities. It typically asks for details about allergies, medications, and any pre-existing medical conditions. This way, staff can be prepared to handle emergencies or specific health needs, making it crucial for participants' well-being.
Another document comparable to the CAPF 160 is the Patient Health Questionnaire (PHQ-9). This form is used in medical settings to assess mental health conditions, particularly depression. Like the CAPF 160, it requires individuals to answer questions about their health history and current issues. The information gathered helps healthcare providers tailor their approach to treatment and support, ensuring that patients receive the most appropriate care based on their unique circumstances.
The Pre-Participation Physical Evaluation (PPE) form is also quite similar to the CAPF 160. This document is commonly required for athletes before they can participate in sports. It collects information about a participant's medical history, physical conditions, and any past injuries. By doing so, the PPE ensures that athletes are fit to engage in physical activities and helps coaches and medical staff identify any potential risks that could affect performance or safety.
Lastly, the Authorization for Medical Treatment form shares similarities with the CAPF 160. This document is often used by parents or guardians to grant permission for medical treatment for minors. Like the CAPF 160, it includes consent for emergency medical care and outlines specific health information that caregivers need to know. This ensures that, in case of an emergency, healthcare providers can act quickly and effectively, prioritizing the health and safety of the child.
When filling out the CAPF 160 form, there are important dos and don'ts to keep in mind. Following these guidelines can help ensure that the information provided is accurate and useful.
Misconceptions about the CAPF 160 form can lead to confusion and miscommunication regarding health and safety. Here are nine common misconceptions clarified:
Understanding these misconceptions can help ensure that all participants are prepared and safe during their activities.
When filling out the CAPF 160 form, it is crucial to provide accurate and complete information. Here are some key takeaways to keep in mind:
Completing the CAPF 160 form with care ensures that the cadet receives appropriate support and medical attention when needed. Take the time to review each section carefully before submission.