The Annual Physical Examination form serves as a comprehensive tool that guides both patients and healthcare providers through the critical components of a yearly health assessment. It begins with essential personal details, including the individual’s name, date of birth, and contact information, ensuring that the medical team has accurate data for follow-up and review. A thorough medical history is crucial; hence, the form requests information about any existing diagnoses, significant health conditions, and current medications. This section helps the physician tailor the examination to the patient’s unique health needs. Patients are also prompted to disclose allergies and sensitivities, which is vital for safe treatment decisions. The form further includes a detailed immunization history, capturing vaccinations such as tetanus, flu shots, and more, so that immunization records are up to date. Tuberculosis screening and other diagnostic tests play a significant role in preventive health care, and their results enhance the physician’s understanding of the patient’s medical landscape. Finally, the examination section evaluates vital signs like blood pressure and heart rate, alongside a complete review of various body systems, ensuring that no aspect of health is overlooked. By taking the time to complete this form thoroughly, individuals streamline their healthcare experience and contribute to more personalized and effective medical care.
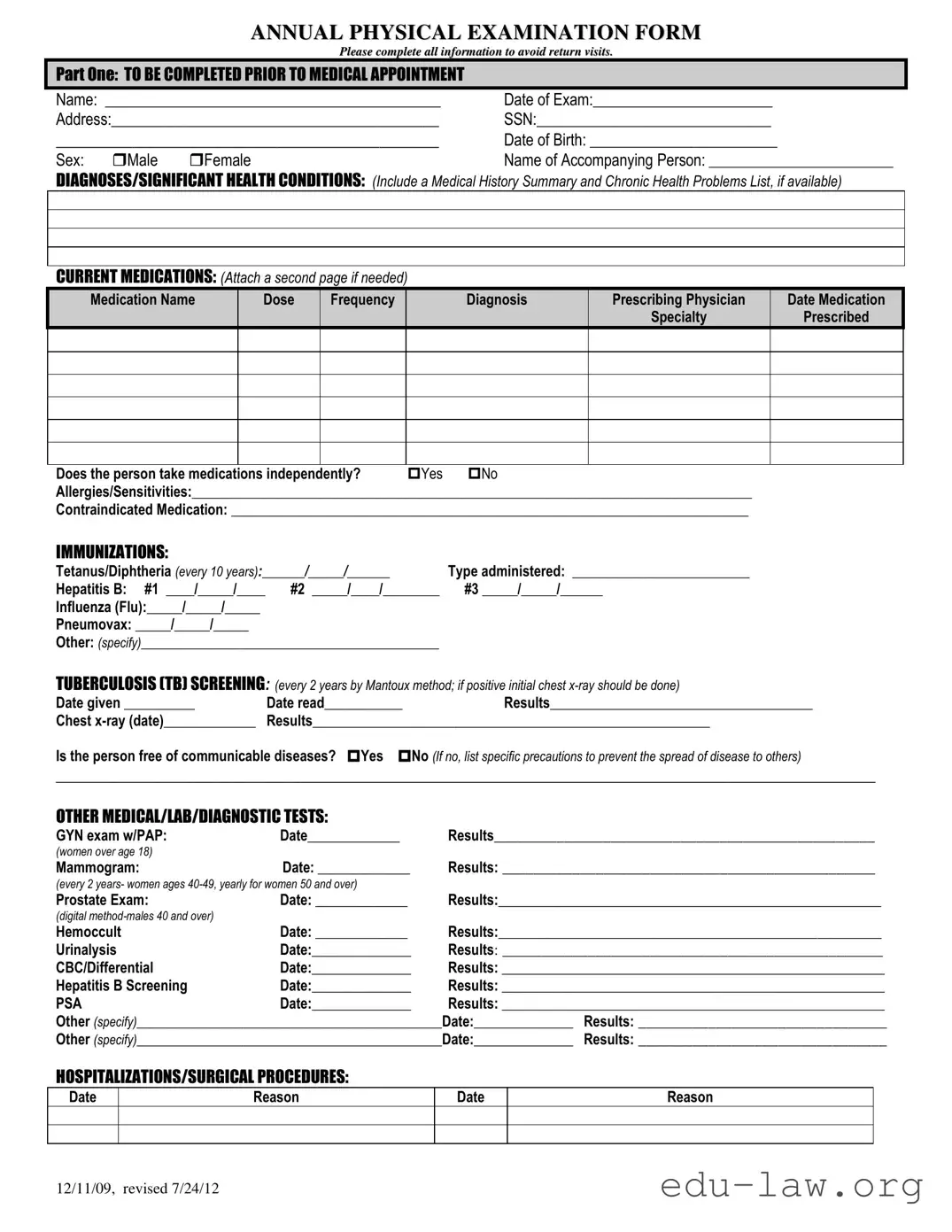
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12
PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12

| Fact Name | Description |
|---|---|
| Purpose of the Form | The Annual Physical Examination Form is designed to gather comprehensive health information about a patient prior to their medical appointment. |
| Required Information | Patients are required to provide personal details such as name, address, date of birth, and medical history to avoid delays during the appointment. |
| Immunization Records | The form includes sections for recording immunization dates and types, ensuring that patients are up to date on their vaccinations. |
| Legal Guidelines | In states like California, the governing laws for patient medical records can be found under the California Health and Safety Code. |
| Evaluation of Systems | The form provides a checklist for evaluating various body systems, enabling healthcare providers to assess normal versus abnormal findings effectively. |
After gathering the necessary information for your Annual Physical Examination form, you can proceed to fill it out. This form helps ensure your healthcare provider has all relevant details before your visit, potentially improving the quality of care you receive. Below are the steps to guide you through completing the form accurately.
What is the purpose of the Annual Physical Examination form?
The Annual Physical Examination form is designed to gather essential health information before your medical appointment. This allows healthcare providers to review your medical history, current medications, allergies, and any significant health conditions. By completing this form, you help ensure that your examination is thorough and tailored to your specific health needs, which can improve the quality of care you receive.
What information do I need to provide in the personal details section?
In the personal details section of the form, you will need to provide your name, date of the examination, address, Social Security number, date of birth, and sex. You should also list the name of any accompanying person. This information is crucial for identification purposes and helps your healthcare provider keep accurate records of your medical history.
Why is it important to disclose my current medications?
Disclosing your current medications is vital for several reasons. First, it helps your healthcare provider understand what treatments you are currently undergoing. This information can prevent potential drug interactions and ensure that any new medications or treatments prescribed during your examination will complement your existing regimen. If needed, you can attach additional pages to provide a complete list of medications, including their dosages and prescribing physicians.
What should I note regarding my immunization history?
When filling out your immunization history, it's important to provide dates and types of vaccines received. This includes vaccinations for tetanus/diphtheria, hepatitis B, influenza, and pneumonia, among others. Knowing your immunization status helps your health provider determine if any additional vaccines are needed to keep you protected against preventable diseases, especially if you are due for a booster or have missed any shots.
How does the form help assess my overall health status?
The Annual Physical Examination form includes sections that assess your vital signs, system evaluations, and any recent medical tests. Healthcare providers can gain valuable insights into your overall health through this information. For instance, documenting blood pressure, weight, and results of tests allows for trend analysis, which can highlight any areas of concern or improvement. This comprehensive approach enables healthcare providers to recommend appropriate interventions, lifestyle modifications, and preventive measures to enhance your health.
Incomplete Personal Information: One common mistake people make is not filling out all the required personal details. This includes name, date of birth, and address. Missing any of these can cause delays in processing your paperwork.
Overlooking Current Medications: Many individuals forget to list all medications they're currently taking. It's crucial to provide an accurate list, including dosages and prescribing physicians, to ensure proper care. Omitting this information can lead to potentially harmful drug interactions.
Neglecting to Update Immunizations: It's a mistake to leave the immunization section incomplete. Failing to record recent vaccinations can result in unnecessary follow-ups or missed opportunities for preventative care.
Ignoring Medical History: People often skip detailing their medical history or significant health conditions. This information is vital for the healthcare provider to understand your background, assess risks, and tailor their recommendations appropriately.
The Annual Physical Examination form is an important document that helps healthcare providers evaluate a person's health status. Along with this form, several other documents and forms are commonly used to gather comprehensive health information. Here’s a brief overview of some of these documents:
These documents work together to provide a comprehensive view of a patient's health and assist in delivering proactive and personalized medical care.
The Annual Wellness Visit form shares similarities with the Comprehensive Health History form. Both documents aim to gather detailed information about a patient’s medical history, including chronic conditions and medications. The Comprehensive Health History form includes personal information and encourages patients to report their existing health issues and medications. This emphasis on thorough background information aids healthcare providers in making informed decisions regarding treatment and preventive measures.
Another document that closely resembles the Annual Physical Examination form is the Medication Management Record. Just like the Physical Examination form, this record ensures that healthcare providers have a complete list of current medications, dosages, and prescribing physicians. By reviewing this information during visits, practitioners can adjust medications appropriately and monitor for potential drug interactions. Both documents significantly contribute to maintaining accurate and comprehensive patient records.
The Preventive Services Checklist also stands in parallel with the Annual Physical Examination form. This checklist is used to track whether patients receive age-appropriate screenings, immunizations, and preventative services. It highlights the importance of vaccination records and identifies necessary tests, echoing many areas addressed in the Annual Physical Examination form. By facilitating the identification of medical needs, both documents play vital roles in patient health maintenance.
Lastly, the Patient Assessment Questionnaire bears similarity to the Annual Physical Examination form due to its focus on evaluating patients' overall health. It typically includes questions about lifestyle factors like diet, exercise, and mental health, in addition to physiological measurements. Both forms provide healthcare providers with an intuitive framework to assess patient well-being holistically, ensuring no critical areas of health are overlooked. This comprehensive approach promotes better health management strategies tailored to individual needs.
When filling out the Annual Physical Examination form, consider the following tips:
Misconceptions about the Annual Physical Examination form can lead to misunderstandings regarding its purpose and use. Here are eight common misconceptions clarified.
The Annual Physical Examination form is a crucial document that facilitates effective healthcare. Here are key takeaways to consider when filling out and utilizing this form:
By carefully filling out this form, individuals contribute to a more efficient and targeted healthcare experience.
Miscellaneous Information - This form is often used by small businesses to report payments to vendors.
Accident Report Form Pdf - Encourage honest and complete responses to ensure effective reporting.