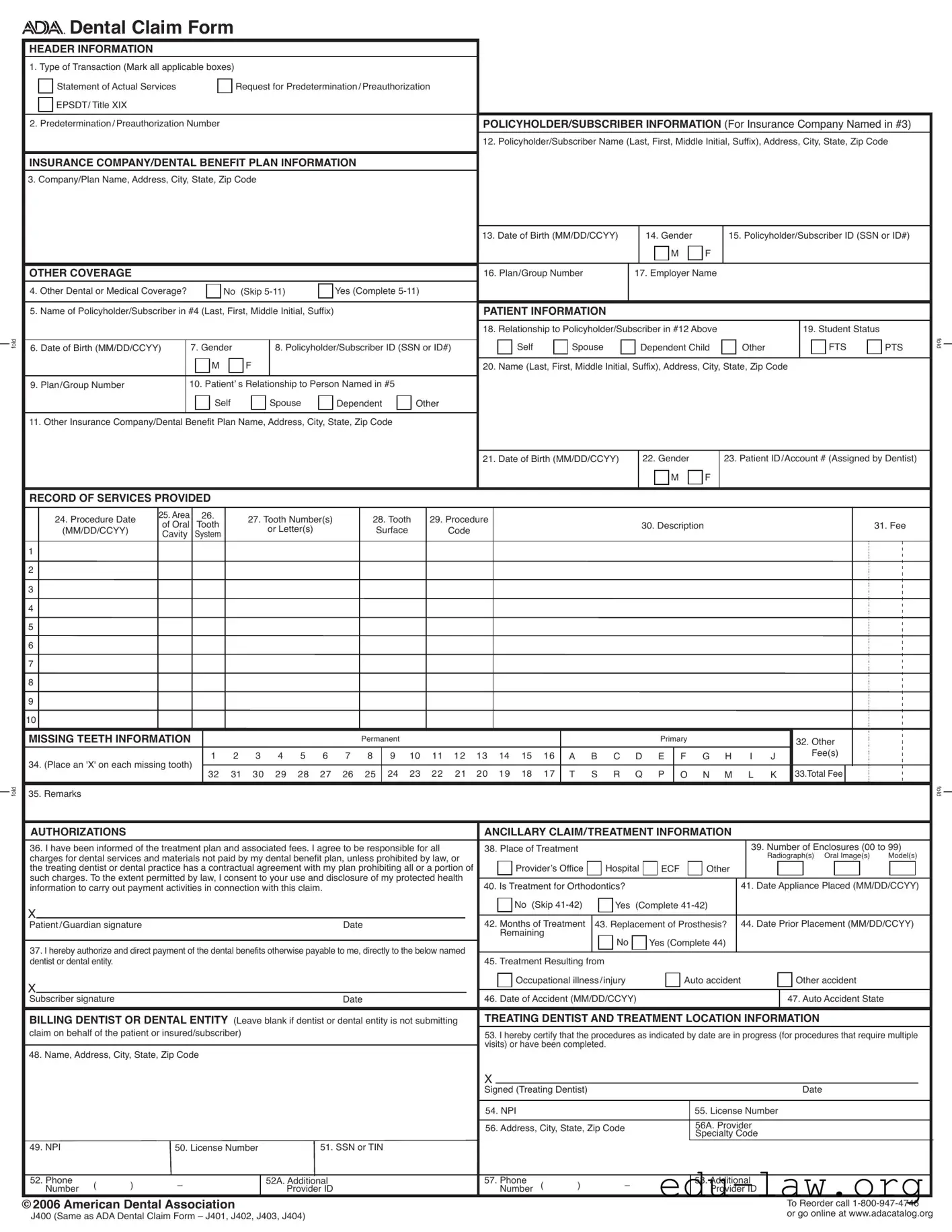
The ADA Dental Claim Form is an essential document for both dental providers and patients navigating the insurance landscape. This form streamlines the process of submitting claims for dental services, ensuring that all necessary information is collected efficiently. It includes sections for header information, such as the type of transaction being requested—whether it's a statement of actual services or a request for predetermination. The form requires detailed policyholder and patient information, including names, addresses, and identification numbers. Additionally, it captures records of services provided, detailing procedures, dates, and associated fees. A critical aspect is the authorization section, where patients acknowledge their understanding of treatment plans and agree to payment responsibilities. Furthermore, the form addresses coordination of benefits for those with multiple insurance coverages, ensuring that all claims are processed accurately. By following the comprehensive guidelines laid out in the form, dental professionals can facilitate smoother transactions and enhance patient experiences.
fold
fold
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
| Fact Name | Description |
|---|---|
| Form Purpose | The ADA Dental Claim Form is used to submit claims for dental services to insurance companies or dental benefit plans. |
| Required Information | All sections of the form must be completed, including details about the policyholder, patient, and services provided, unless specified otherwise. |
| National Provider Identifier (NPI) | The form requires the NPI of the dentist or dental entity submitting the claim. This identifier is essential for HIPAA compliance. |
| State-Specific Laws | Different states may have specific regulations governing the use of the ADA Dental Claim Form, which may include requirements for additional documentation or specific submission processes. |
Filling out the ADA Dental Claim Form is an important step in ensuring that dental services are billed correctly to your insurance provider. This process requires attention to detail and accuracy to avoid delays in processing your claim. Follow these steps to complete the form properly.
What is the purpose of the ADA Dental Claim Form?
The ADA Dental Claim Form is designed to facilitate the submission of dental claims to insurance companies or dental benefit plans. It collects essential information about the patient, the policyholder, and the dental services provided. By using this form, dental practices can ensure that claims are processed efficiently and accurately, helping patients receive the benefits they are entitled to.
How do I complete the header information section?
In the header information section, you will need to indicate the type of transaction. Mark all applicable boxes, such as "Statement of Actual Services" or "Request for Predetermination/Preauthorization." Additionally, you should provide the predetermination or preauthorization number if applicable. Make sure to fill in the policyholder or subscriber's name, address, and other required details to ensure proper identification of the claim.
What should I do if the patient has other dental or medical coverage?
If the patient has other dental or medical coverage, you must complete the designated sections of the form. This includes providing the name of the policyholder for the other coverage and any relevant plan or group numbers. If there is no other coverage, simply skip to the next section. Accurate reporting of all insurance information helps in coordinating benefits and ensuring that claims are processed correctly.
How do I report the services provided on the claim form?
To report the services provided, fill in the "Record of Services Provided" section. Include the procedure date, area, tooth numbers, procedure codes, and a description of the services rendered. It is essential to list all relevant procedures accurately. If the number of procedures exceeds the available lines on the form, use an additional claim form to report the remaining services.
What is the significance of the National Provider Identifier (NPI)?
The National Provider Identifier (NPI) is a unique identifier assigned to healthcare providers, including dentists, by the federal government. It is crucial for the claim submission process as it helps identify the provider of the services rendered. Ensure that you include the NPI in the appropriate sections of the claim form to facilitate accurate processing of the claim by the insurance company.
What should I do if I need to submit a claim to a secondary payer?
When submitting a claim to a secondary payer, it is important to complete the form in its entirety. You must attach the primary payer’s Explanation of Benefits (EOB) that shows the amount paid by the primary payer. Additionally, you can indicate the amount paid by the primary carrier in the "Remarks" field. This information is vital for the secondary payer to process the claim correctly and efficiently.
Incomplete Header Information: Failing to mark all applicable transaction types can lead to delays or denials. Ensure that you check all boxes that apply, such as "Statement of Actual Services" or "Request for Predetermination."
Missing Policyholder Information: Omitting the complete name and address of the policyholder can result in processing issues. Always include the full name, address, and other required details.
Incorrect Patient Information: Providing inaccurate patient details, such as date of birth or relationship to the policyholder, can lead to claim rejections. Double-check all patient information for accuracy.
Neglecting Other Coverage: If there is additional dental or medical coverage, failing to complete the relevant sections can affect claim processing. Always indicate whether there is other coverage and provide the necessary details.
Improperly Documenting Services Provided: Incomplete or unclear descriptions of procedures, such as missing tooth numbers or procedure codes, can lead to confusion. Ensure all services are thoroughly documented.
Missing Signatures: Not signing the claim form can halt the processing of your claim. Both the patient/guardian and the treating dentist must sign where indicated.
Ignoring Coordination of Benefits: If submitting to a secondary payer, failing to attach the primary payer’s Explanation of Benefits (EOB) can result in claim denials. Always include necessary documentation.
Incorrect Use of Dates: Omitting the four-digit year in date fields can lead to errors. Always use the full date format, including the year, to avoid processing issues.
When submitting a dental claim, the ADA Dental Claim Form is just one of several important documents that may be required. Each of these documents serves a specific purpose in the claims process, ensuring that all necessary information is provided for proper evaluation and payment. Below is a list of additional forms and documents often used alongside the ADA Dental Claim Form.
Understanding these additional forms can help streamline the dental claims process. By ensuring that all necessary documentation is submitted, patients and dental providers can work together effectively to facilitate timely reimbursement and minimize delays.
The ADA Dental Claim Form shares similarities with the CMS-1500 form, which is used for medical claims. Both forms require detailed information about the patient, the insurance policyholder, and the services provided. Each form has sections for identifying the provider and the patient’s relationship to the policyholder. Additionally, both forms allow for the inclusion of multiple insurance coverages, ensuring that all relevant information is submitted for processing claims efficiently.
Another document comparable to the ADA Dental Claim Form is the UB-04 form, commonly used for hospital billing. Like the dental claim form, the UB-04 captures essential details about the patient, the provider, and the services rendered. Both forms require precise coding to describe the procedures performed. They also include sections for additional coverage information, which aids in coordinating benefits between multiple insurers.
The Health Insurance Claim Form (HICF) is another document that resembles the ADA Dental Claim Form. This form is used for various types of health insurance claims and requires similar demographic information about the patient and policyholder. Both forms emphasize the need for accurate procedure codes and billing details, ensuring that the claims are processed correctly by the insurance companies.
The Workers' Compensation Claim Form is similar in that it also collects information regarding the patient, the provider, and the services rendered. This form is specifically designed for claims related to workplace injuries. Like the ADA Dental Claim Form, it requires details about the insurance coverage and the nature of the treatment, facilitating a smoother claims process for both the provider and the patient.
The Medicare Dental Claim Form is another document that aligns closely with the ADA Dental Claim Form. It serves a similar purpose in submitting claims for dental services covered under Medicare. Both forms require patient and provider information, as well as detailed descriptions of the services provided. They also facilitate the submission of claims to ensure that patients receive the benefits they are entitled to under their insurance plans.
The Medicaid Dental Claim Form is comparable as it is specifically tailored for claims submitted to Medicaid programs. Like the ADA form, it collects comprehensive information about the patient, the provider, and the services provided. Both forms have sections dedicated to documenting other insurance coverage, which is crucial for coordinating benefits and ensuring that claims are processed accurately.
The Dental Treatment Plan form shares similarities with the ADA Dental Claim Form in that it outlines the proposed dental services and associated costs. Both documents require detailed patient information and consent for treatment. While the treatment plan focuses on the planned services, the claim form is used to request payment for those services after they have been provided.
The Explanation of Benefits (EOB) is another document that relates to the ADA Dental Claim Form. While the EOB provides a summary of what services were billed and what payments were made, it complements the claim form by showing the outcome of the claim submission. Both documents are essential for understanding the financial aspects of dental care and insurance coverage.
The Prior Authorization Request form is similar to the ADA Dental Claim Form in that it seeks approval for specific dental services before they are provided. Both forms require detailed patient and provider information, along with descriptions of the services requested. They are both critical in ensuring that patients receive the necessary treatments covered by their insurance plans.
Finally, the Dental Referral Form is akin to the ADA Dental Claim Form in that it includes information about the patient and the services needed. While the referral form is used to direct patients to specialists, it often accompanies the claim submission process. Both forms ensure that all relevant details are communicated effectively, supporting continuity of care for the patient.
When filling out the ADA Dental Claim Form, attention to detail is crucial. Here are ten important do's and don'ts to keep in mind:
By following these guidelines, you can help ensure that your claim is processed smoothly and efficiently.
Here are some common misconceptions about the ADA Dental Claim Form:
When filling out and using the ADA Dental Claim Form, it is essential to keep several key points in mind to ensure a smooth submission process. Here are nine important takeaways:
By following these guidelines, you can help ensure that your dental claims are processed efficiently and accurately.